

Analysis of guidelines for screening diabetes mellitus in an ambulatory population
- PMID: 20042558
- PMCID: PMC2800288
- DOI: 10.4065/mcp.2009.0289
Analysis of guidelines for screening diabetes mellitus in an ambulatory population
Abstract
Objectives: To compare the case-finding ability of current national guidelines for screening diabetes mellitus and characterize factors that affect testing practices in an ambulatory population.
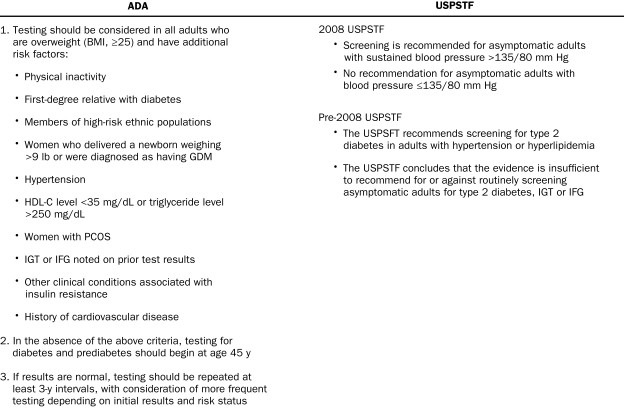
Patients and methods: In this retrospective analysis, we reviewed a database of 46,991 nondiabetic patients aged 20 years and older who were seen at a large Midwestern academic physician practice from January 1, 2005, through December 31, 2007. Patients were included in the sample if they were currently being treated by the physician group according to Wisconsin Collaborative for Healthcare Quality criteria. Pregnant patients, diabetic patients, and patients who died during the study years were excluded. The prevalence of patients who met the American Diabetes Association (ADA) and/or US Preventive Services Task Force (USPSTF) criteria for diabetes screening, percentage of these patients screened, and number of new diabetes diagnoses per guideline were evaluated. Screening rates were assessed by number of high-risk factors, primary care specialty, and insurance status.
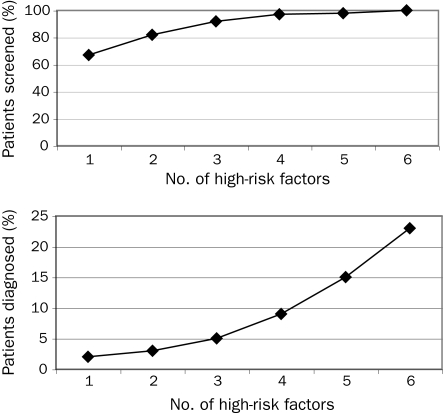
Results: A total of 33,823 (72.0%) of 46,991 patients met either the ADA or the USPSTF screening criteria, and 28,842 (85.3%) of the eligible patients were tested. More patients met the ADA criteria than the 2008 USPSTF criteria (30,790 [65.5%] vs 12,054 [25.6%]), and the 2008 USPSTF guidelines resulted in 460 fewer diagnoses of diabetes (33.1%). By single high-risk factor, prediabetes (15.8%) and polycystic ovarian syndrome (12.6%) produced the highest rates of diagnosis. The number of ADA high-risk factors predicted diabetes, with 6 (23%) of 26 patients with 6 risk factors diagnosed as having diabetes. Uninsured patients were tested significantly less often than insured patients (54.9% vs 85.4%).
Conclusion: Compared with the ADA recommendations, the new USPSTF guidelines result in a lower number of patients eligible for screening and decrease case finding significantly. The number and type of risk factors predict diabetes, and lack of health insurance decreases testing.
Figures
References
-
- Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and impaired fasting glucose in adults in the U.S. population: National Health and Nutrition Examination Survey 1999-2002. Diabetes Care 2006;29(6):1263-1268 - PubMed
-
- Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S., 2005-2050. Diabetes Care 2006;29(9):2114-2116 - PubMed
-
- Harris MI, Klein R, Welborn TA, Knuiman MW. Onset of NIDDM occurs at least 4-7 yr before clinical diagnosis. Diabetes Care 1992;15(7):815-819 - PubMed
-
- Nathan DM, Cleary PA, Backlund JY, et al. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643-2653 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
