

Organization-wide adoption of computerized provider order entry systems: a study based on diffusion of innovations theory
- PMID: 20043843
- PMCID: PMC2809050
- DOI: 10.1186/1472-6947-9-52
Organization-wide adoption of computerized provider order entry systems: a study based on diffusion of innovations theory
Abstract
Background: Computerized provider order entry (CPOE) systems have been introduced to reduce medication errors, increase safety, improve work-flow efficiency, and increase medical service quality at the moment of prescription. Making the impact of CPOE systems more observable may facilitate their adoption by users. We set out to examine factors associated with the adoption of a CPOE system for inter-organizational and intra-organizational care.
Methods: The diffusion of innovation theory was used to understand physicians' and nurses' attitudes and thoughts about implementation and use of the CPOE system. Two online survey questionnaires were distributed to all physicians and nurses using a CPOE system in county-wide healthcare organizations. The number of complete questionnaires analyzed was 134 from 200 nurses (67.0%) and 176 from 741 physicians (23.8%). Data were analyzed using descriptive-analytical statistical methods.
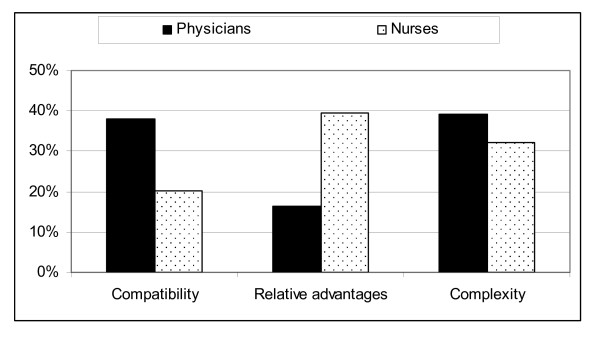
Results: More nurses (56.7%) than physicians (31.3%) stated that the CPOE system introduction had worked well in their clinical setting (P < 0.001). Similarly, more physicians (73.9%) than nurses (50.7%) reported that they found the system not adapted to their specific professional practice (P = < 0.001). Also more physicians (25.0%) than nurses (13.4%) stated that they did want to return to the previous system (P = 0.041). We found that in particular the received relative advantages of the CPOE system were estimated to be significantly (P < 0.001) higher among nurses (39.6%) than physicians (16.5%). However, physicians' agreements with the compatibility of the CPOE and with its complexity were significantly higher than the nurses (P < 0.001).
Conclusions: Qualifications for CPOE adoption as defined by three attributes of diffusion of innovation theory were not satisfied in the study setting. CPOE systems are introduced as a response to the present limitations in paper-based systems. In consequence, user expectations are often high on their relative advantages as well as on a low level of complexity. Building CPOE systems therefore requires designs that can provide rather important additional advantages, e.g. by preventing prescription errors and ultimately improving patient safety and safety of clinical work. The decision-making process leading to the implementation and use of CPOE systems in healthcare therefore has to be improved. As any change in health service settings usually faces resistance, we emphasize that CPOE system designers and healthcare decision-makers should continually collect users' feedback about the systems, while not forgetting that it also is necessary to inform the users about the potential benefits involved.
Figures
References
-
- Kohn LT, Corrigan JM, Donaldson MS, editors. To err is human: building a safer health system. Washington DC: Institute of Medicine report. National Academies Press; 1999. - PubMed
-
- Bates DW, Kuperman G, Teich JM. Computerized physician order entry and quality of care. Qual Manag Health Care. 1994;2(4):18–27. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
