

HIV-1 neuroimmunity in the era of antiretroviral therapy
- PMID: 20044002
- PMCID: PMC2840259
- DOI: 10.1016/j.nbd.2009.12.015
HIV-1 neuroimmunity in the era of antiretroviral therapy
Abstract
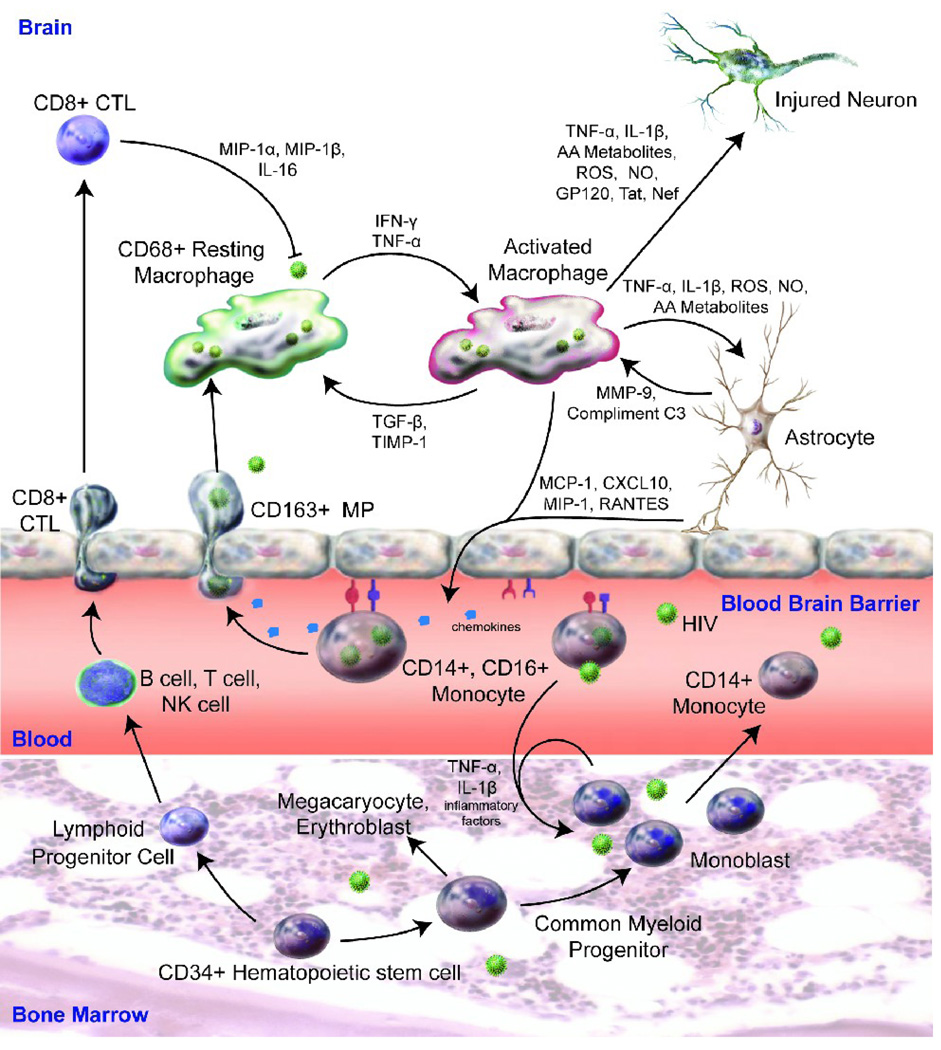
Human immunodeficiency virus type 1 (HIV-1)-associated neurocognitive disorders (HAND) can affect up to 50% of infected people during the disease course. While antiretroviral therapies have substantively increased the quality of life and reduced HIV-1-associated dementia, less severe minor cognitive and motor deficits continue. Trafficking of HIV-1 into the central nervous system (CNS), peripheral immune activation, dysregulated glial immunity, and diminished homeostatic responses are the disease-linked pathobiologic events. Monocyte-macrophage passage into the CNS remains an underlying force for disease severity. Monocyte phenotypes may change at an early stage of cell maturation and immune activation of hematopoietic stem cells. Activated monocytes are pulled into the brain in response to chemokines made as a result of glial inflammatory processes, which in turn, cause secondary functional deficits in neurons. Current therapeutic approaches are focused on adjunctive and brain-penetrating antiretroviral therapies. These may attenuate virus-associated neuroinflammatory activities thereby decreasing the severity and frequency of HAND.
2009 Elsevier Inc. All rights reserved.
Figures
References
-
- Achmat Z, Simcock J. Combining prevention, treatment and care: lessons from South Africa. Aids. 2007;21(Suppl 4):S11–20. - PubMed
-
- Aline F, et al. Dendritic cells loaded with HIV-1 p24 proteins adsorbed on surfactant-free anionic PLA nanoparticles induce enhanced cellular immune responses against HIV-1 after vaccination. Vaccine. 2009;27:5284–5291. - PubMed
-
- Ances BM, Ellis RJ. Dementia and neurocognitive disorders due to HIV-1 infection. Semin Neurol. 2007;27(1):86–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 NS036126/NS/NINDS NIH HHS/United States
- P01 NS043985/NS/NINDS NIH HHS/United States
- R01NS034239/NS/NINDS NIH HHS/United States
- P01 NS031492/NS/NINDS NIH HHS/United States
- P01 NS31492/NS/NINDS NIH HHS/United States
- R37 NS036126/NS/NINDS NIH HHS/United States
- P20 RR015635/RR/NCRR NIH HHS/United States
- R01 NS034239/NS/NINDS NIH HHS/United States
- P01 NS43985/NS/NINDS NIH HHS/United States
- P01 MH057556/MH/NIMH NIH HHS/United States
- R37 NS36126/NS/NINDS NIH HHS/United States
- P01 DA026146/DA/NIDA NIH HHS/United States
- P20RR15635/RR/NCRR NIH HHS/United States
- P01 MH064570/MH/NIMH NIH HHS/United States
- R01 NS036127/NS/NINDS NIH HHS/United States
- T32 NS007488/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
