

Deferoxamine treatment for intracerebral hemorrhage in aged rats: therapeutic time window and optimal duration
- PMID: 20044521
- PMCID: PMC2896218
- DOI: 10.1161/STROKEAHA.109.569830
Deferoxamine treatment for intracerebral hemorrhage in aged rats: therapeutic time window and optimal duration
Abstract
Background and purpose: Deferoxamine (DFX) reduces brain edema, neurological deficits, and brain atrophy after intracerebral hemorrhage (ICH) in aged and young rats. Our previous study found that 50 mg/kg is an effective dose in aged rats. In the present study, we explored potential therapeutic time windows and optimal therapeutic durations.
Methods: Aged male Fischer 344 rats (18 months old) sustained an intracaudate injection of 100 microL autologous whole blood, followed by intramuscular DFX or vehicle beginning at different time points, or continuing for different durations. Subgroups of rats were euthanized at day 3 for brain edema measurement and day 56 for brain atrophy determination. Behavioral tests were performed on days 1, 28, and 56 after ICH.
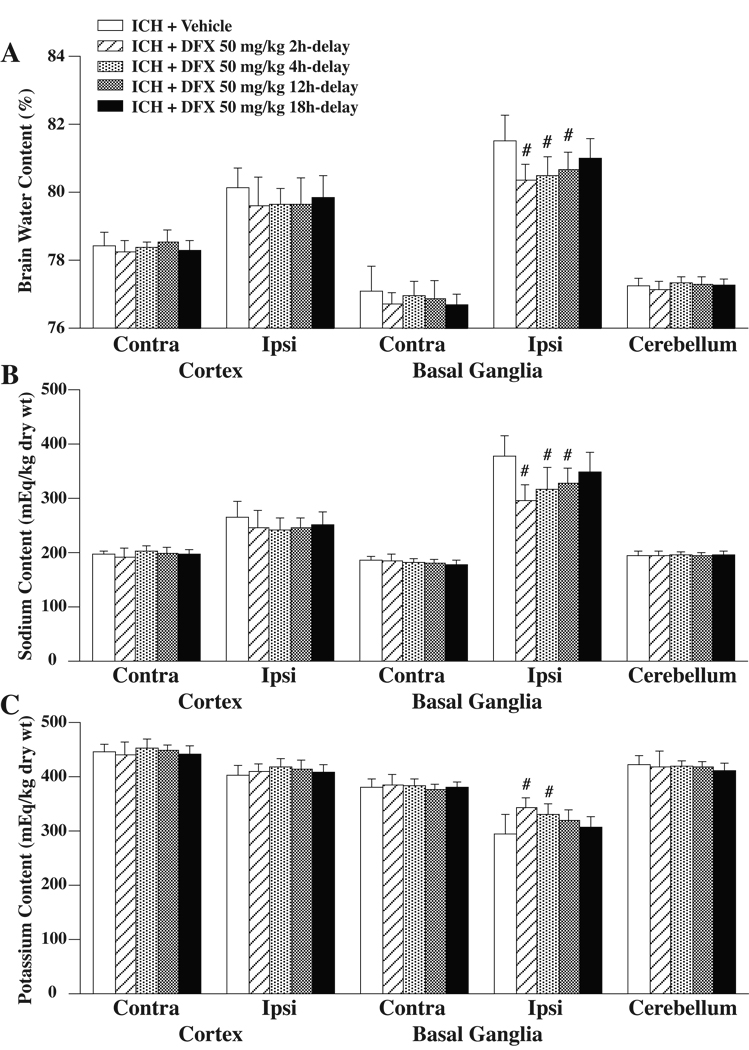
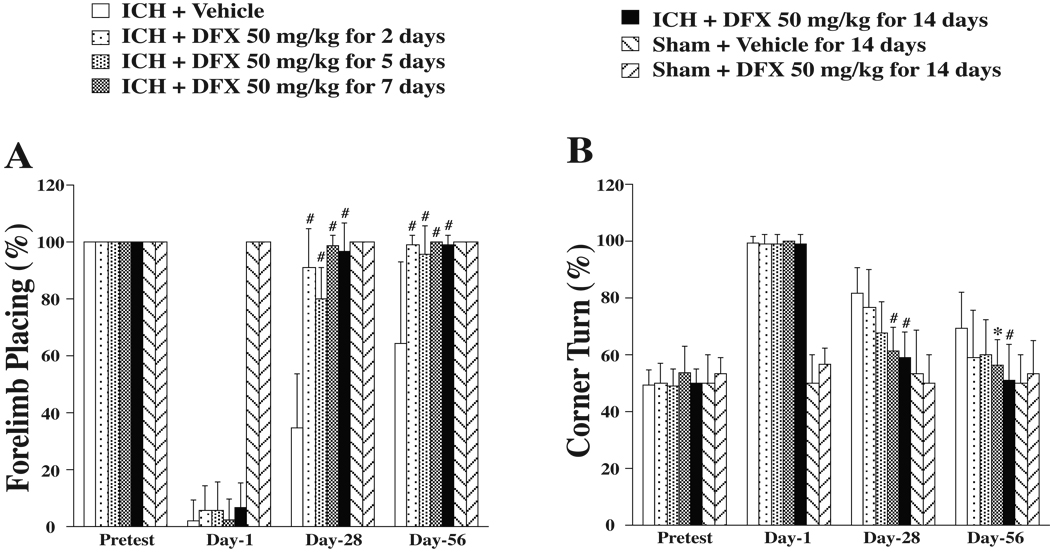
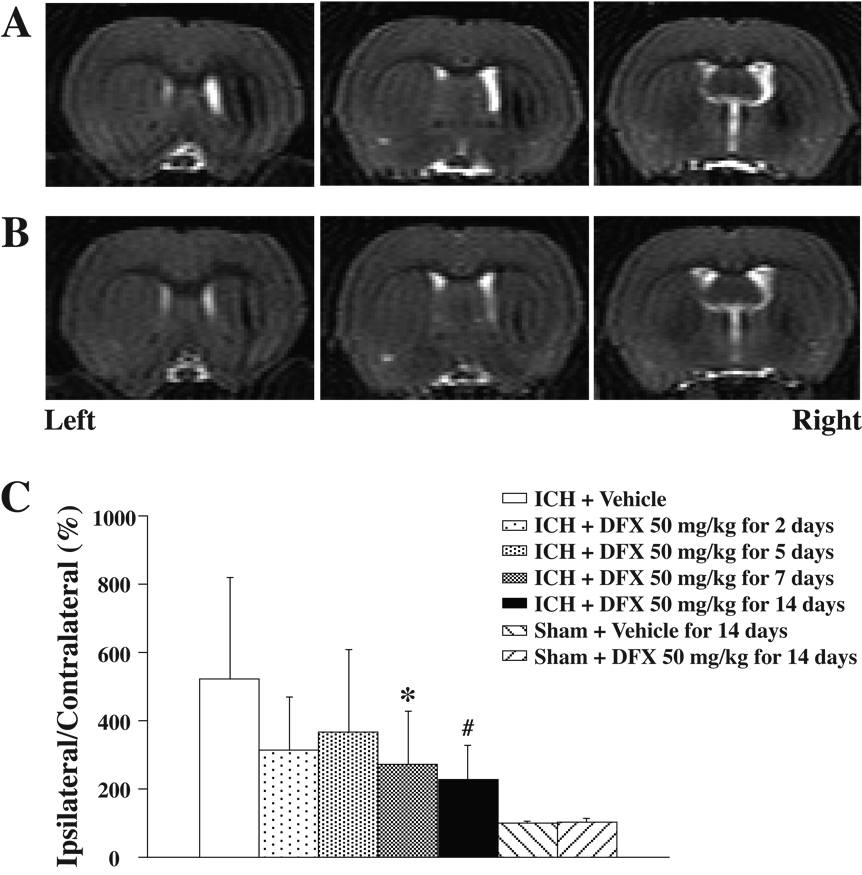
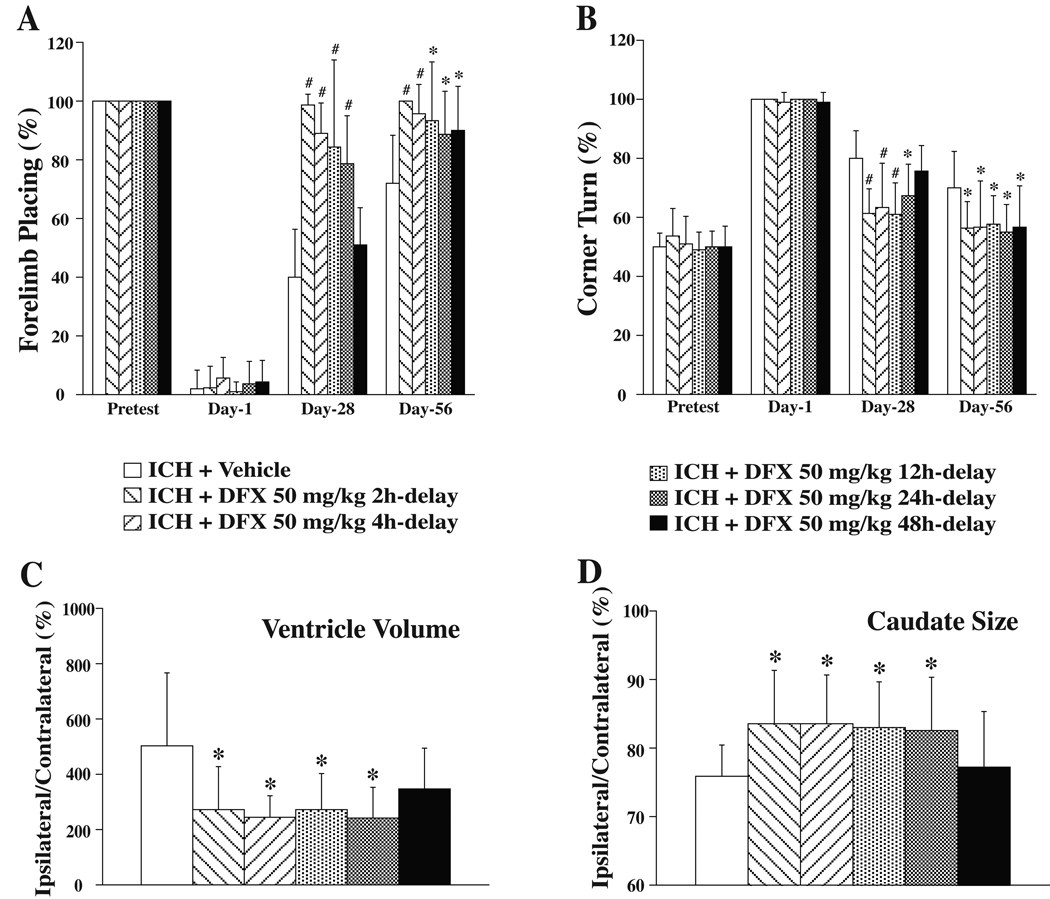
Results: Systemic administration of DFX, when begun within 12 hours after ICH, reduced brain edema. DFX treatment started 2 hours after ICH and administered for >or=7 days attenuated ICH-induced ventricle enlargement, caudate atrophy, and neurological deficits. DFX attenuated ICH-induced brain atrophy and neurological deficits without detectable side effects when begun within 24 hours and administered for 7 days.
Conclusions: To the extent that these results can be translated to humans, the therapeutic time window and the optimal duration for DFX in this aged rat model of ICH may provide useful information for an ongoing DFX-ICH clinical trial.
Figures

References
-
- Broderick JP, Brott T, Tomsick T, Miller R, Huster G. Intracerebral hemorrhage more than twice as common as subarachnoid hemorrhage. J Neurosurg. 1993;78:188–191. - PubMed
-
- Xi G, Keep RF, Hoff JT. Mechanisms of brain injury after intracerebral hemorrhage. Lancet Neurol. 2006;5:53–63. - PubMed
-
- Wu J, Hua Y, Keep RF, Nakamura T, Hoff JT, Xi G. Iron and iron-handling proteins in the brain after intracerebral hemorrhage. Stroke. 2003;34:2964–2969. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
