

Protamine reduces bleeding complications associated with carotid endarterectomy without increasing the risk of stroke
- PMID: 20045609
- PMCID: PMC5240820
- DOI: 10.1016/j.jvs.2009.10.078
Protamine reduces bleeding complications associated with carotid endarterectomy without increasing the risk of stroke
Abstract
Objectives: Controversy persists regarding the use of protamine during carotid endarterectomy (CEA) based on prior conflicting reports documenting both reduced bleeding as well as increased stroke risk. The purpose of this study was to determine the effect of protamine reversal of heparin anticoagulation on the outcome of CEA in a contemporary multistate registry.
Methods: We reviewed a prospective regional registry of 4587 CEAs in 4311 patients performed by 66 surgeons from 11 centers in Northern New England from 2003-2008. Protamine use varied by surgeon (38% routine use, 44% rare use, 18% selective use). Endpoints were postoperative bleeding requiring reoperation as well as potential thrombotic complications, including stroke, death, and myocardial infarction (MI). Predictors of endpoints were determined by multivariate logistic regression after associated variables were identified by univariate analysis.
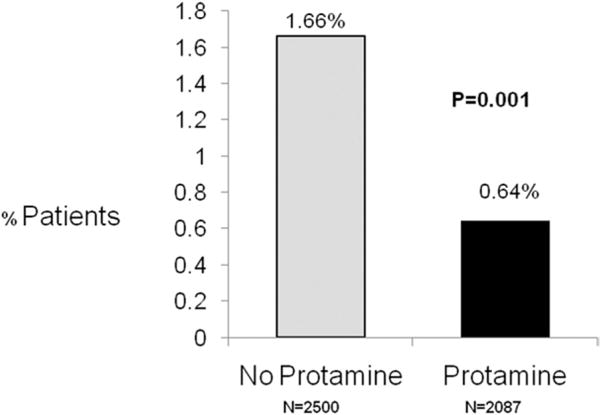
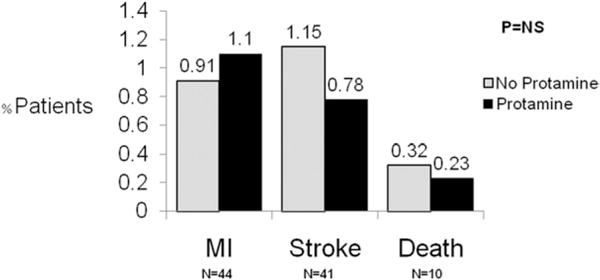
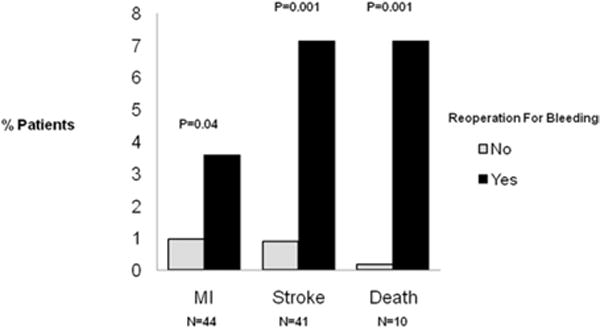
Results: Of the 4587 CEAs performed, 46% utilized protamine, while 54% did not. Fourteen patients (0.64%) in the protamine-treated group required reoperation for bleeding compared with 42 patients (1.66%) in the untreated cohort (P = .001). Protamine use did not affect the rate of MI (1.1% vs 0.91%, P = .51), stroke (0.78% vs 1.15%, P = .2), or death (0.23% vs 0.32%, P = .57) between treated and untreated patients, respectively. By multivariate analysis, protamine (odds ratio [OR] 0.32, 95% confidence interval [CI], 0.17-0.63; P = .001) and patch angioplasty (OR 0.46, 95% CI, 0.26-0.81; P = .007) were independently associated with diminished reoperation for bleeding. A single center was associated with a significantly higher rate of reoperation for bleeding (OR 6.47, 95% CI, 3.02-13.9; P < .001). Independent of protamine use, consequences of reoperation for bleeding were significant, with a four-fold increase in MI, a seven-fold increase in stroke, and a 30-fold increase in death.
Conclusion: Protamine reduced serious bleeding requiring reoperation during CEA without increasing the risk of MI, stroke, or death, in this large, contemporary registry. In light of significant complications referable to bleeding, liberal use of protamine during CEA appears warranted.
Conflict of interest statement
Competition of interest: none.
Figures
References
-
- Riles TS, Imparato AM, Jacobowitz GR, Lamparello PJ, Giangola G, Adelman MA, Landis R. The cause of perioperative stroke after carotid endarterectomy. J Vasc Surg. 1994;19:206–14. discussion 215–6. - PubMed
-
- Weber CF, Friedl H, Hueppe M, Hintereder G, Schmitz-Rixen T, Zwissler B, Meininger D. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg. 2009;33:1526–32. - PubMed
-
- Lutz HJ, Michael R, Gahl B, Savolainen H. Local versus general anaesthesia for carotid endarterectomy-improving the gold standard? Eur J Vasc Endovasc Surg. 2008;36:145–9. disussion 150–1. - PubMed
-
- AbuRahma AF, Stone PA, Elmore M, Flaherty SK, Armistead L, Abu-Rahma Z. Prospective randomized trial of ACUSEAL (Gore-Tex) vs Finesse (Hemashield) patching during carotid endarterectomy: long-term outcome. J Vasc Surg. 2008;48:99–103. - PubMed
-
- Naylor R, Hayes PD, Payne DA, Allroggen H, Steel S, Thompson MM, et al. Randomized trial of vein versus dacron patching during carotid endarterectomy: long-term results. J Vasc Surg. 2004;39:985–93. discussion 993. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
