

Strategies to reduce early morbidity and mortality in adults receiving antiretroviral therapy in resource-limited settings
- PMID: 20046144
- PMCID: PMC3772276
- DOI: 10.1097/COH.0b013e328333850f
Strategies to reduce early morbidity and mortality in adults receiving antiretroviral therapy in resource-limited settings
Abstract
Purpose of review: We review recently published literature concerning early morbidity and mortality during antiretroviral therapy (ART) among patients in resource-limited settings. We focus on articles providing insights into this burden of disease and strategies to address it.
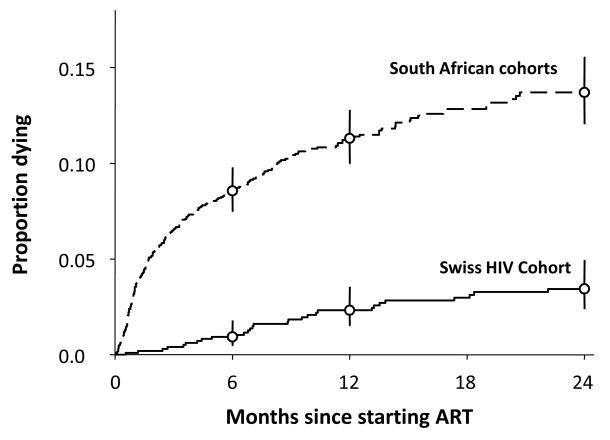
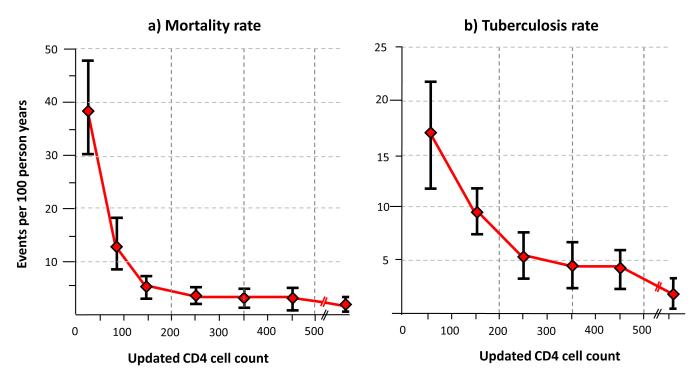
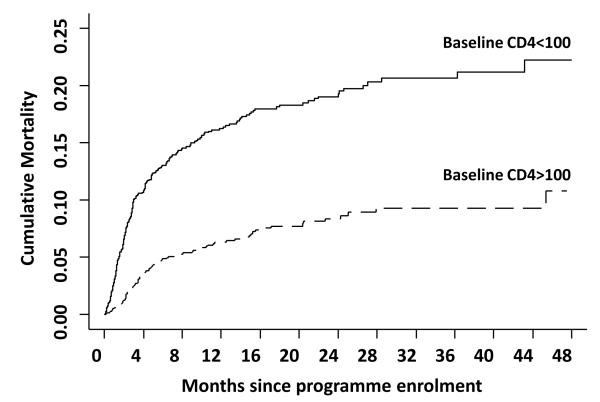
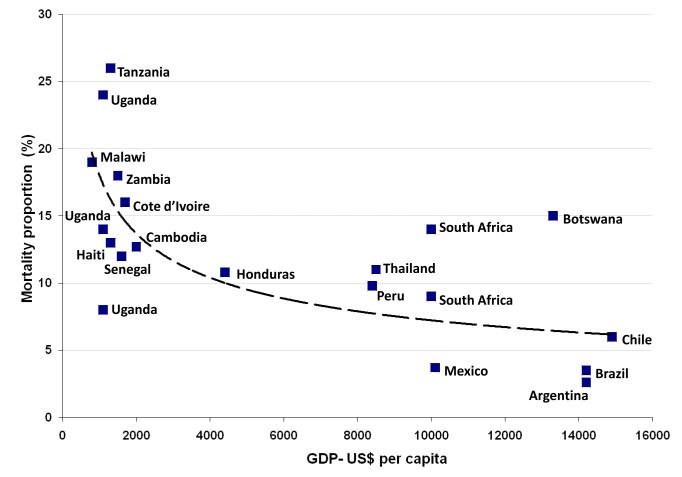
Recent findings: In sub-Saharan Africa, mortality rates during the first year of ART are very high (8-26%), with most deaths occurring in the first few months. This figure compares with 3-13% in programmes in Latin America and the Caribbean and 11-13% in south-east Asia. Risk factors generally reflect late presentation with advanced symptomatic disease. Key causes of morbidity and mortality include tuberculosis (TB), acute sepsis, cryptococcal meningitis, malignancy and wasting syndrome/chronic diarrhoea. Current literature shows that the fundamental need is for much earlier HIV diagnosis and initiation of ART. In addition, further studies provide data on the role of screening and prophylaxis against opportunistic diseases (particularly TB, bacterial sepsis and cryptococcal disease) and the management of specific opportunistic diseases and complications of ART. Effective and sustainable delivery of these interventions requires strengthening of programmes.
Summary: Strategies to address this disease burden should include earlier HIV diagnosis and ART initiation, screening and prophylaxis for opportunistic infections, optimized management of specific diseases and treatment complications, and programme strengthening.
Figures
References
-
- UNAIDS . 2008 Report on the global AIDS epidemic. UNAIDS; Geneva: 2008. Available at: http://www.unaids.org/en/KnowledgeCentre/HIVData/GlobalReport/2008/2008_....
-
- World Health Organization . Progress report 2008. World Health Organization; Geneva: 2008. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector. Accessible at: http://www.who.int/entity/hiv/pub/towards_universal_access_report_2008.pdf.
-
- Souteyrand Y, Akwara P, Warner Smith M, et al. Scaling up access to antiretroviral therapy (ART) in low- and middle-income countries: global and regional progress in 2008. Abstracts of the 5th International AIDS Society conference on HIV pathogenesis, treatment and prevention; Cape Town, South Africa. International AIDS Society; Jul, 2009. Abstract WELBD105.
-
- Braitstein P, Brinkhof MW, F Dabis, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–24. - PubMed
-
-
Lawn SD, Harries AD, Anglaret X, Myer L, Wood R. Early mortality among adults accessing antiretroviral treatment programmes in sub-Saharan Africa. AIDS. 2008;22:1897–908. A comprehensive of the mortality rates (8%-26% in the first year) risk factors, causes and potential interventions to address this in ART programmes in sub-Saharan Africa.
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
