

Management of individuals requiring antiretroviral therapy and TB treatment
- PMID: 20046149
- PMCID: PMC2936963
- DOI: 10.1097/COH.0b013e3283339309
Management of individuals requiring antiretroviral therapy and TB treatment
Abstract
Purpose of review: Globally, tuberculosis (TB) is the commonest opportunistic infection in people living with HIV. Many co-infected patients first present with advanced immunosuppression and require antiretroviral therapy (ART) initiation during TB treatment. The incidence of TB in patients established on ART remains high. Co-treatment presents several management challenges. Recent data on these management issues are reviewed.
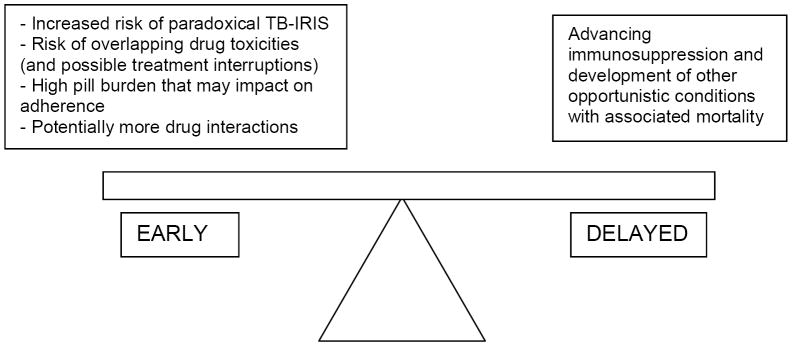
Recent findings: Efavirenz concentrations at standard doses are similar with and without concomitant rifampicin-based TB treatment. Nevirapine concentrations are frequently subtherapeutic during lead-in dosing at 200 mg daily in patients on rifampicin-based TB treatment, which may result in inferior virological outcomes. Hepatotoxicity occurred in three pharmacokinetic studies (conducted in healthy volunteers) of boosted protease inhibitors initiated in participants on rifampicin. Results of a clinical trial comparing efavirenz-based and nevirapine-based ART in patients on TB treatment, with no lead-in dosing of nevirapine, are awaited. Concurrent TB treatment increases the need for stavudine substitutions, mainly related to neuropathy. Consensus case definitions for TB immune reconstitution inflammatory syndrome (TB-IRIS) have been published. It is important to exclude TB drug resistance in patients with suspected TB-IRIS. A clinical trial demonstrated benefit of prednisone for treating TB-IRIS, reducing a combined endpoint of days of hospitalization and outpatient therapeutic procedures. Starting ART during TB treatment improved survival in patients with CD4 cell count less than 500 cells/mul, but the optimal interval between starting TB treatment and starting ART remains to be determined in several ongoing trials.
Summary: ART improves survival in co-infected TB patients, but is complicated by several management challenges that compromise programmatic implementation in resource-limited settings. Recent findings and the findings of ongoing studies will assist clinicians in dealing with these challenges.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Lawn SD, Myer L, Bekker LG, Wood R. Burden of tuberculosis in an antiretroviral treatment programme in sub-Saharan Africa: impact on treatment outcomes and implications for tuberculosis control. AIDS. 2006;20:1605–12. - PubMed
-
- Baalwa J, Mayanja-Kizza H, Kamya MR, et al. Worsening and unmasking of tuberculosis in HIV-1 infected patients after initiating highly active anti-retroviral therapy in Uganda. Afr Health Sci. 2008;8:190–5. - PMC - PubMed
-
A study from a Ugandan ART cohort that reports the incidence, timing and clinical manifestations of paradoxical TB-IRIS and incident TB on ART.
-
- Scano F, Vitoria M, Burman W, et al. Management of HIV-infected patients with MDR-and XDR-TB in resource-limited settings. Int J Tuberc Lung Dis. 2008;12:1370–5. - PubMed
-
A review article of management issues in patients with HIV and drug resistant TB (MDR and XDR) in resource limited settings.
-
- Coyne KM, Pozniak AL, Lamorde M, Boffito M. Pharmacology of second-line antituberculosis drugs and potential for interactions with antiretroviral agents. AIDS. 2009;23:437–46. - PubMed
-
A review of the pharmacology of drugs used for the treatment of drug-resistant TB with specific emphasis on potential drug interactions and shared toxicities with antiretroviral agents.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
