

Congenital rickets caused by maternal vitamin D deficiency
- PMID: 20046322
- PMCID: PMC2795674
- DOI: 10.1093/pch/7.7.455
Congenital rickets caused by maternal vitamin D deficiency
Abstract
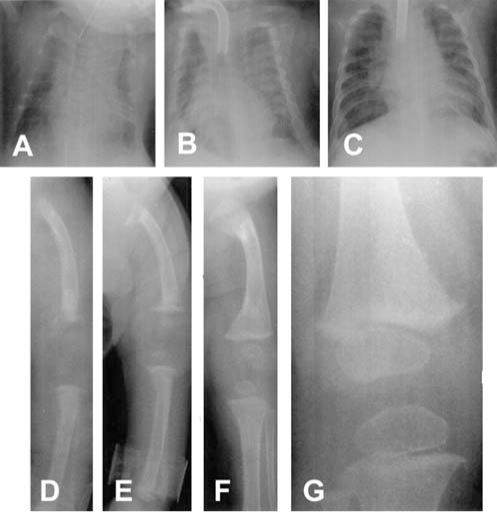
The cases of four newborn infants with congenital rickets are reported. All infants were native Canadian: three were Cree and one was Inuit. One had a narrow chest and pulmonary hypoplasia, two had clinical and radiological signs of rickets with craniotabes, thickened wrists, and prominent costochondral junctions, and one had perinatal asphyxia and hydrops. All had hypocalcemia, hypophosphatemia and secondary hyperparathyroidism. Serum 25-hydroxyvitamin D levels were low in three of the infants. The four mothers had evidence of vitamin D deficiency. All infants recovered following treatment with 5000 IU oral vitamin D daily.
On rend compte du cas de quatre nouveau-nés atteints de rachitisme congénital. Tous étaient originaires du Canada. Trois étaient Cris et un, Inuit. L’un avait le thorax étroit et une hypoplasie pulmonaire, deux présentaient des signes cliniques et radiologiques de rachitisme accompagné de craniotabès, de poignets épaissis et d’un chapelet costal, et le dernier souffrait d’asphyxie périnatale et d’anasarque. Tous étaient atteints d’hypocalcémie, d’hypophosphatémie et d’hyperparathyroïdie secondaire. Le taux de 25-hydroxyvitamine D sérique était faible chez trois des nouveau-nés. Les quatre mères manifestaient des signes de carence en vitamine D. Tous les enfants se sont rétablis après un traitement quotidien de 5 000 UI de vitamine D par voie orale.
Keywords: 25-hydroxyvitamin D; Congenital rickets; Hyperparathyroidism; Hypocalcemia.
Figures
Similar articles
-
Congenital rickets due to vitamin D deficiency in the mothers.Clin Nutr. 2015 Oct;34(5):793-8. doi: 10.1016/j.clnu.2014.12.006. Epub 2014 Dec 17. Clin Nutr. 2015. PMID: 25552383 Review.
-
Craniotabes in Newborns and the Role of Maternal Vitamin D Deficiency: A Case Series.Cureus. 2024 Nov 15;16(11):e73730. doi: 10.7759/cureus.73730. eCollection 2024 Nov. Cureus. 2024. PMID: 39677085 Free PMC article.
-
Hypocalcemic seizures in breastfed infants with rickets secondary to severe maternal vitamin D deficiency.Pak J Biol Sci. 2010 May 1;13(9):437-42. doi: 10.3923/pjbs.2010.437.442. Pak J Biol Sci. 2010. PMID: 20973397
-
Oral Supplementation of Parturient Mothers with Vitamin D and Its Effect on 25OHD Status of Exclusively Breastfed Infants at 6 Months of Age: A Double-Blind Randomized Placebo Controlled Trial.Breastfeed Med. 2017 Dec;12(10):621-628. doi: 10.1089/bfm.2016.0164. Epub 2017 Oct 13. Breastfeed Med. 2017. PMID: 29027817 Clinical Trial.
-
The Return of Congenital Rickets, Are We Missing Occult Cases?Calcif Tissue Int. 2016 Sep;99(3):227-36. doi: 10.1007/s00223-016-0146-2. Epub 2016 May 31. Calcif Tissue Int. 2016. PMID: 27245342 Review.
Cited by
-
Bone metabolism in the fetus and neonate.Pediatr Nephrol. 2014 May;29(5):793-803. doi: 10.1007/s00467-013-2461-4. Epub 2013 Mar 26. Pediatr Nephrol. 2014. PMID: 23529641 Review.
-
Effect of Vitamin D Supplementation in Early Life on Children's Growth and Body Composition: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Nutrients. 2021 Feb 5;13(2):524. doi: 10.3390/nu13020524. Nutrients. 2021. PMID: 33562750 Free PMC article.
-
Neonatal Severe Hyperparathyroidism: Novel Insights From Calcium, PTH, and the CASR Gene.J Clin Endocrinol Metab. 2020 Apr 1;105(4):1061-78. doi: 10.1210/clinem/dgz233. J Clin Endocrinol Metab. 2020. PMID: 31778168 Free PMC article.
-
Bone development in the fetus and neonate: role of the calciotropic hormones.Curr Osteoporos Rep. 2011 Dec;9(4):274-83. doi: 10.1007/s11914-011-0073-0. Curr Osteoporos Rep. 2011. PMID: 21904825 Review.
-
Vitamin D, rickets and child abuse: controversies and evidence.Pediatr Radiol. 2021 May;51(6):1014-1022. doi: 10.1007/s00247-020-04893-w. Epub 2021 May 17. Pediatr Radiol. 2021. PMID: 33999242 Review.
References
-
- Haworth JC, Dilling LA, deGroot W, Greenberg CR, Longstaffe SEA, Moffatt MEK. Vitamin D deficiency in Manitoba and northwest Ontario. Can J Pediatr. 1995;2:331–5.
-
- Fraser D, Kooh SW, Kind HP, Holick MF, Tanaka Y, DeLuca HF. Pathogenesis of hereditary vitamin-D-dependent rickets. An inborn error of vitamin D metabolism involving defective conversion of 25-hydroxyvitamin D to 1a, 25-dihydroxyvitamin D. N Engl J Med. 1973;289:817–22. - PubMed
-
- Brooks MH, Bell NH, Love L, et al. Vitamin-D-dependent rickets type II. Resistance of target organs to 1,25-dihydroxyvitamin D. N Engl J Med. 1978;298:996–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources