

Hospitalization of children with acute immune thrombocytopenic purpura - is it necessary?
- PMID: 20046330
- PMCID: PMC2795686
- DOI: 10.1093/pch/7.6.386
Hospitalization of children with acute immune thrombocytopenic purpura - is it necessary?
Abstract
Objective: To identify a target group of children with acute immune thrombocytopenic purpura (ITP) that may not require hospitalization for management.
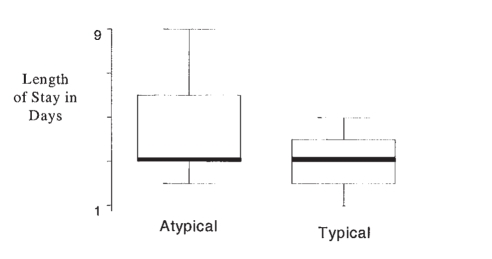
Methods: A retrospective chart review was conducted of all children admitted over a two-year period to a tertiary care paediatric hospital with the diagnosis of acute ITP. Patients were classified according to typical and atypical presentations. Typical patients were defined as those aged between one and 10 years, with no hepatomegaly or significant splenomegaly and who had typical laboratory features for ITP. Patients who did not meet these criteria were categorized as atypical. Outcome measures included length of stay (LOS) in hospital; frequency of bone marrow aspiration (BMA); type of treatment; incidence of intracranial hemorrhage (ICH) or severe bleeding; and admission and discharge platelet counts.
Results: There were 74 patients hospitalized for a mean of 3.6 days. No patients suffered an ICH or bleeding requiring transfusion. Patients with typical presentations (42) were compared with patients with atypical presentations (32) and were not significantly different for clinically important outcomes such as admission and discharge platelet counts, serious complications or type of therapy. Typical patients had significantly fewer BMAs than did atypical patients - 22 of 42 (52%) versus 25 of 32 (78%) (P=0.02), and a shorter LOS - 3.1 (+/-0.9) days versus 4.2 (+/-1.8) days (P=0.01).
Conclusions: Children presenting with ITP have a low incidence of bleeding complications and many of these patients can be managed as outpatients. A multicentre study is needed to properly delineate a low risk group suited for outpatient medical management.
OBJECTIF :: Repérer un groupe cible d’enfants atteints d’un purpura thrombopénique immun (PTI) aigu qui n’ont peutêtre pas besoin d’être hospitalisés pour être pris en charge.
MÉTHODOLOGIE :: L’étude rétrospective de dossiers médicaux de tous les enfants admis à un hôpital de soins tertiaires pédiatriques en raison d’un diagnostic de PTI aigu a été effectuée relativement à une période de deux ans. Les patients ont été classés selon les présentations types ou atypiques. Les patients types ont été définis comme des enfants de un à dix ans, sans splénomégalie grave ou hépatomégalie et qui présentaient des caractéristiques de laboratoire types de PTI. Les patients qui ne respectaient pas ces critères ont été classés comme atypiques. Les mesures d’issue incluaient la durée de l’hospitalisation (DH), la fréquence de ponction de moelle osseuse (PMO), le type de traitement, l’incidence d’hémorragie intracrânienne (HI) ou une grave hémorragie, de même que la numération plaquettaire à l’hospitalisation et au congé.
RÉSULTATS :: Soixante-quatorze patients ont été hospitalisés pendant une période moyenne de 3,6 jours. Aucun ne souffrait d’HI ou d’hémorragie exigeant une transfusion. Les patients affichant une présentation type (42) ont été comparés à ceux affichant une présentation atypique (32), et les résultats ne différaient pas de manière considérable pour ce qui est de la numération plaquettaire à l’admission et au congé, des complications graves ou du type de traitement. Les patients types présentaient beaucoup moins de PMO que les patients atypiques, soit 22 sur 42 (52 %) par rapport à 25 sur 32 (78 %) (P=0,02), et une DH plus courte, de 3,1 (±0,9) jours par rapport à 4,2 (±1,8) jours (P=0,01).
CONCLUSIONS :: Les enfants qui se présentent avec un PTI affichent une incidence peu élevée de complications avec saignements, et bon nombre de ces patients peuvent être pris en charge sur une base ambulatoire. Une étude multicentre s'impose pour bien délimiter un groupe à faible risque convenant à une prise en charge médicale ambulatoire.
Keywords: Hospitalization; Immune thrombocytopenic purpura; Treatment.
Figures
Similar articles
-
Impact of immune thrombocytopenic purpura on clinical outcomes in patients with acute myocardial infarction.Clin Cardiol. 2020 Jan;43(1):50-59. doi: 10.1002/clc.23287. Epub 2019 Nov 11. Clin Cardiol. 2020. PMID: 31710764 Free PMC article.
-
Idiopathic thrombocytopenic purpura: a 10-year natural history study at the childrens hospital of alabama.Clin Pediatr (Phila). 2004 Oct;43(8):691-702. doi: 10.1177/000992280404300802. Clin Pediatr (Phila). 2004. PMID: 15494875
-
Is bone marrow aspiration needed in acute childhood idiopathic thrombocytopenic purpura to rule out leukemia?Arch Pediatr Adolesc Med. 1998 Apr;152(4):345-7. doi: 10.1001/archpedi.152.4.345. Arch Pediatr Adolesc Med. 1998. PMID: 9559709
-
Childhood acute immune thrombocytopenic purpura: 20 years later.Semin Thromb Hemost. 2003 Dec;29(6):605-17. doi: 10.1055/s-2004-815628. Semin Thromb Hemost. 2003. PMID: 14719177 Review.
-
[Idiopathic thrombocytopenic purpura in children].Med Pregl. 1998 Mar-Apr;51(3-4):127-34. Med Pregl. 1998. PMID: 9611955 Review. Croatian.
References
-
- McClure PD. Idiopathic thrombocytopenic purpura in children: Diagnosis and management. Pediatrics. 1975;55:68–74. - PubMed
-
- Bussel JB. Autoimmune thrombocytopenic purpura. Hematol Oncol Clin North Am. 1990;4:179–91. - PubMed
-
- Lusher JM, Emami A, Ravindranath Y, Warrier AI. Idiopathic thrombocytopenic purpura in children: The case for management without steroids. Am J Pediatr Hematol Oncol. 1984;6:149–57. - PubMed
-
- George JN, Woolf SH, Raskob GE, et al. Idiopathic thrombocytopenic purpura: A practice guideline developed by explicit methods for the American Society of Hematology. Blood. 1996;88:3–40. - PubMed
LinkOut - more resources
Full Text Sources