

Preoperative radiologic and postoperative pathologic risk factors for early intra-hepatic recurrence in hepatocellular carcinoma patients who underwent curative resection
- PMID: 20046419
- PMCID: PMC2796405
- DOI: 10.3349/ymj.2009.50.6.789
Preoperative radiologic and postoperative pathologic risk factors for early intra-hepatic recurrence in hepatocellular carcinoma patients who underwent curative resection
Abstract
Purpose: The risk of hepatocellular carcinoma (HCC) recurrence must be considered ahead of surgery. This study was undertaken to identify pre-operative risk factors for early intrahepatic recurrence of HCC after curative resection in a large-scale.
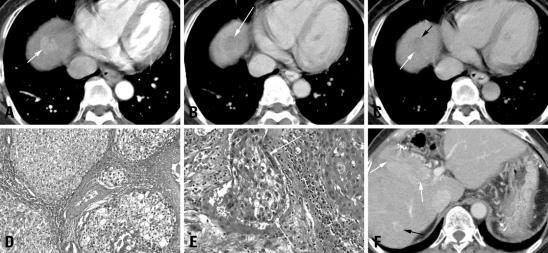
Materials and methods: We retrospectively reviewed the preoperative three-phase multi-detector CT (MDCT) and laboratory data for 240 HCC patients who underwent curative resection; tumor size, number, gross shape, capsule integrity, distinctiveness of tumor margin, portal vein thrombosis (PVT), alpha-fetoprotein level (AFP), and protein induced by vitamin K absence-II (PIVKA-II) levels were assessed. Surgical pathology was reviewed; tumor differentiation, capsule, necrosis, and micro-vessel invasion were recorded.
Results: HCC recurred in 61 patients within six months (early recurrence group), but not in 179 patients (control group). In univariate analysis, large tumor size (p = 0.018), shape (p = 0.028), poor capsule integrity (p = 0.046), elevated AFP (p = 0.015), and PIVKA-II (p = 0.008) were significant preoperative risk factors. Among the pathologic features, PVT (p = 0.023), Glisson's capsule penetration (p = 0.033), microvascular invasion (p < 0.001), and poor differentiation (p = 0.001) showed statistical significance. In multivariate analysis, only the histopathologic parameters of microvascular invasion and poor differentiation achieved statistical significance.
Conclusion: Preoperative CT and laboratory parameters showed limited value, while the presence of microscopic vascular tumor invasion and poorly differentiated HCC correlated with higher risk of early recurrence after curative resection.
Keywords: Hepatocellular carcinoma; curative resection; early recurrence; postoperative pathologic findings; preoperative CT.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Clark HP, Carson WF, Kavanagh PV, Ho CP, Shen P, Zagoria RJ. Staging and current treatment of hepatocellular carcinoma. Radiographics. 2005;25(Suppl 1):S3–S23. - PubMed
-
- Ulmer SC. Hepatocellular carcinoma. A concise guide to its status and management. Postgrad Med. 2000;107:117–124. - PubMed
-
- Ng KK, Vauthey JN, Pawlik TM, Lauwers GY, Regimbeau JM, Belghiti J, et al. Is hepatic resection for large or multinodular hepatocellular carcinoma justified? Results from a multi-institutional database. Ann Surg Oncol. 2005;12:364–373. - PubMed
-
- Mor E, Kaspa RT, Sheiner P, Schwartz M. Treatment of hepatocellular carcinoma associated with cirrhosis in the era of liver transplantation. Ann Intern Med. 1998;129:643–653. - PubMed
-
- Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002;35:519–524. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
