

State-of-the-art CT imaging techniques for congenital heart disease
- PMID: 20046490
- PMCID: PMC2799649
- DOI: 10.3348/kjr.2010.11.1.4
State-of-the-art CT imaging techniques for congenital heart disease
Abstract
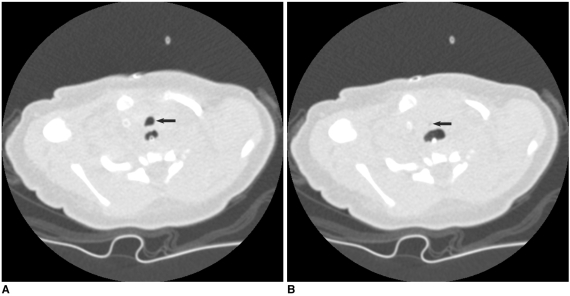
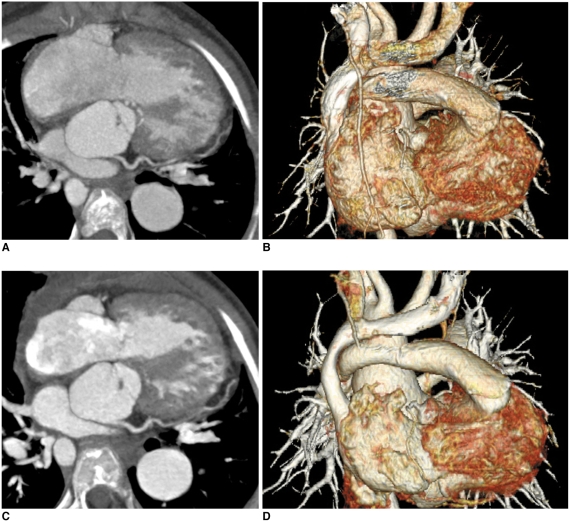
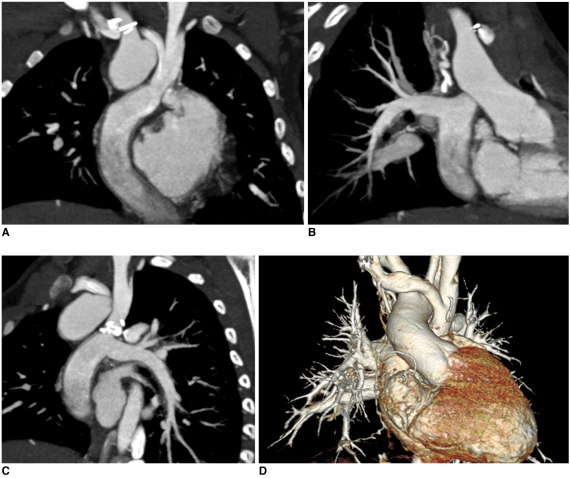
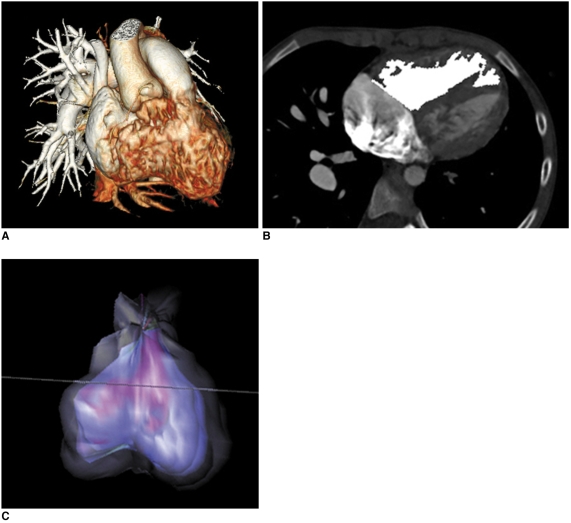
CT is increasingly being used for evaluating the cardiovascular structures and airways in the patients with congenital heart disease. Multi-slice CT has traditionally been used for the evaluation of the extracardiac vascular and airway abnormalities because of its inherent high spatial resolution and excellent air-tissue contrast. Recent developments in CT technology primarily by reducing the cardiac motion and the radiation dose usage in congenital heart disease evaluation have helped expand the indications for CT usage. Tracheobronchomalacia associated with congenital heart disease can be evaluated with cine CT. Intravenous contrast injection should be tailored to unequivocally demonstrate cardiovascular abnormalities. Knowledge of the state-of-the-art CT imaging techniques that are used for evaluating congenital heart disease is helpful not only for planning and performing CT examinations, but also for interpreting and presenting the CT image findings that consequently guide the proper medical and surgical management.
Keywords: Computed tomography (CT) techniques; Congenital heart disease; Multi-slice CT.
Figures

References
-
- Goo HW, Park IS, Ko JK, Kim YH, Seo DM, Yun TJ, et al. CT of congenital heart disease: normal anatomy and typical pathologic conditions. Radiographics. 2003;23:S147–S165. - PubMed
-
- Goo HW, Park IS, Ko JK, Kim YH, Seo DM, Park JJ. Computed tomography for the diagnosis of congenital heart disease in pediatric and adult patients. Int J Cardiovasc Imaging. 2005;21:347–365. - PubMed
-
- Leschka S, Oechslin E, Husmann L, Desbiolles L, Marincek B, Genoni M, et al. Pre- and postoperative evaluation of congenital heart disease in children and adults with 64-section CT. Radiographics. 2007;27:829–846. - PubMed
-
- Goo HW. Pediatric CT: understanding of radiation dose and optimization of imaging techniques. J Korean Radiol Soc. 2005;52:1–5. [Korean]
-
- Yang DH, Goo HW. Pediatric 16-slice CT protocol: radiation dose and image quality. J Korean Radiol Soc. 2008;59:333–347.
