

Central or atypical skull base osteomyelitis: diagnosis and treatment
- PMID: 20046592
- PMCID: PMC2731471
- DOI: 10.1055/s-0028-1115325
Central or atypical skull base osteomyelitis: diagnosis and treatment
Abstract
Objective: We report cases of central or atypical skull base osteomyelitis and review issues related to the diagnosis and treatment.
Methods: The four cases presented, which were drawn from the Oxford, United Kingdom, skull base pathology database, had a diagnosis of central skull base osteomyelitis.
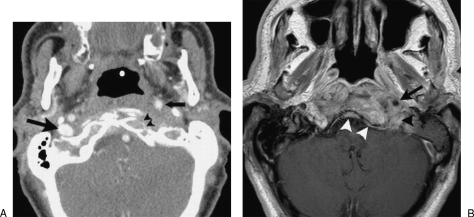
Results: Four cases are presented in which central skull base osteomyelitis was diagnosed. Contrary to malignant otitis externa, our cases were not preceded by immediate external infections and had normal external ear examinations. They presented with headache and a variety of cranial neuropathies. Imaging demonstrated bone destruction, and subsequent microbiological analysis diagnosed infection and prompted prolonged antibiotic treatment.
Conclusion: We concluded that in the diabetic or immunocompromised patient, a scenario of headache, cranial neuropathy, and bony destruction on imaging should raise the possibility of skull base osteomyelitis, even in the absence of an obvious infective source. The primary goal should still be to exclude an underlying malignant cause.
Keywords: Skull base; cranial neuropathies; osteomyelitis; otitis externa.
Figures
References
-
- Cavel O, Fliss D M, Segev Y, Zik D, Khafif A, Landsberg R. The role of the otorhinolaryngologist in the management of central skull base osteomyelitis. Am J Rhinol. 2007;21(3):281–285. - PubMed
-
- Kulkarni S, Lee A, Lee J H. Sixth and tenth nerve palsy secondary to pseudomonas infection of the skull base. Am J Ophthalmol. 2005;139(5):918–920. - PubMed
-
- Keane J R. Combined VIth and XIIth cranial nerve palsies: A clival syndrome. Neurology. 2000;54:1540–1541. - PubMed
-
- Rowlands R G, Lekakis G K, Hinton A E. Masked pseudomonal skull base osteomyelitis presenting with a bilateral Xth cranial nerve palsy. J Laryngol Otol. 2002;116:556–558. - PubMed
-
- Seabold J E, Simonson T M, Weber P C, et al. Cranial osteomyelitis: diagnosis and follow-up with In-111 white blood cell and Tc-99m methylene diphosphonate bone SPECT, CT, and MR imaging. Radiology. 1995;196:779–788. - PubMed
