

The SLIM Study: Slo-Niacin® and Atorvastatin Treatment of Lipoproteins and Inflammatory Markers in Combined Hyperlipidemia
- PMID: 20046930
- PMCID: PMC2757280
- DOI: 10.1016/j.jacl.2009.04.052
The SLIM Study: Slo-Niacin® and Atorvastatin Treatment of Lipoproteins and Inflammatory Markers in Combined Hyperlipidemia
Abstract
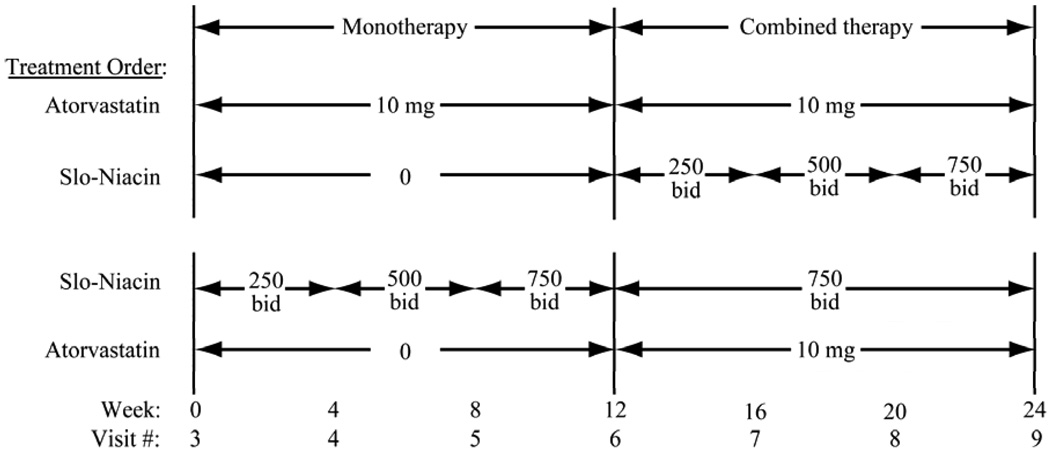
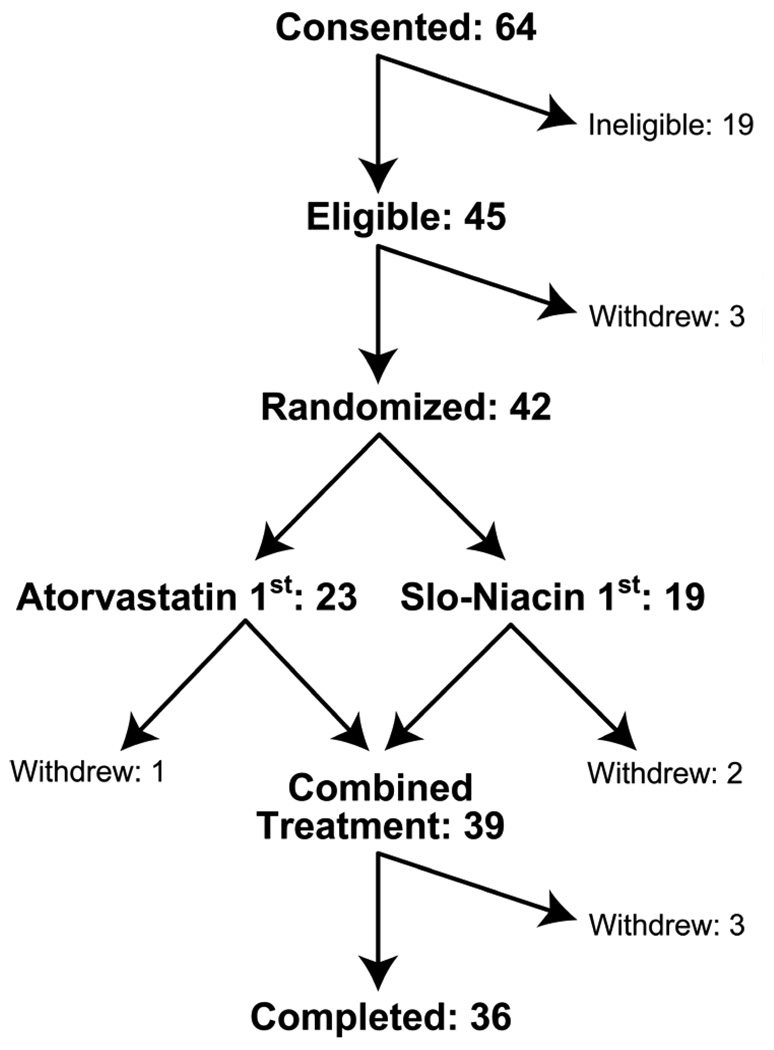
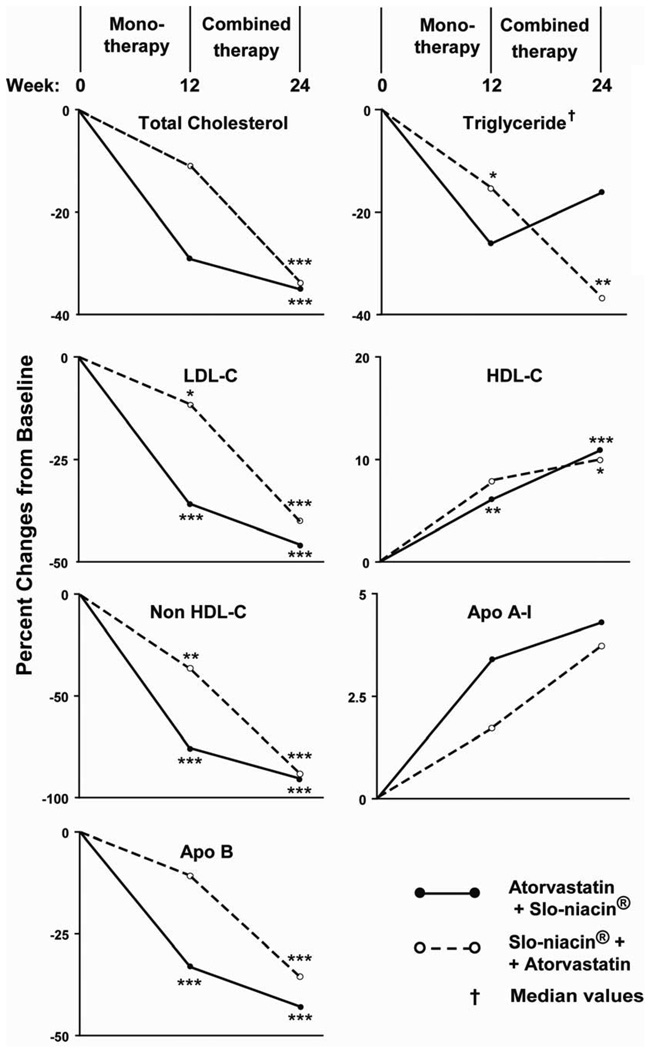
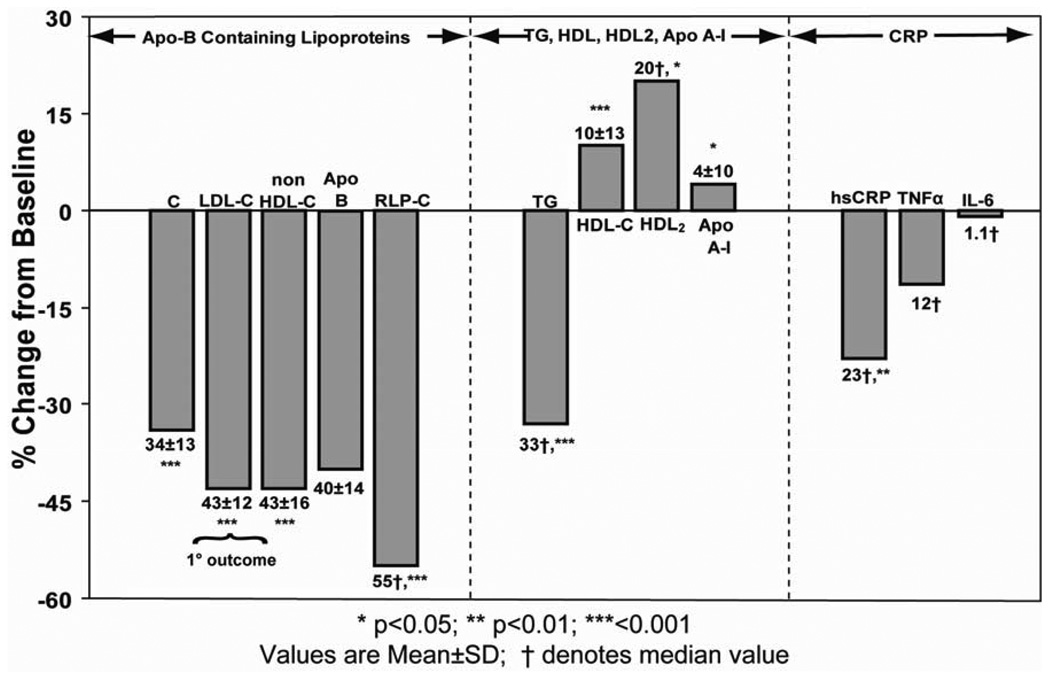
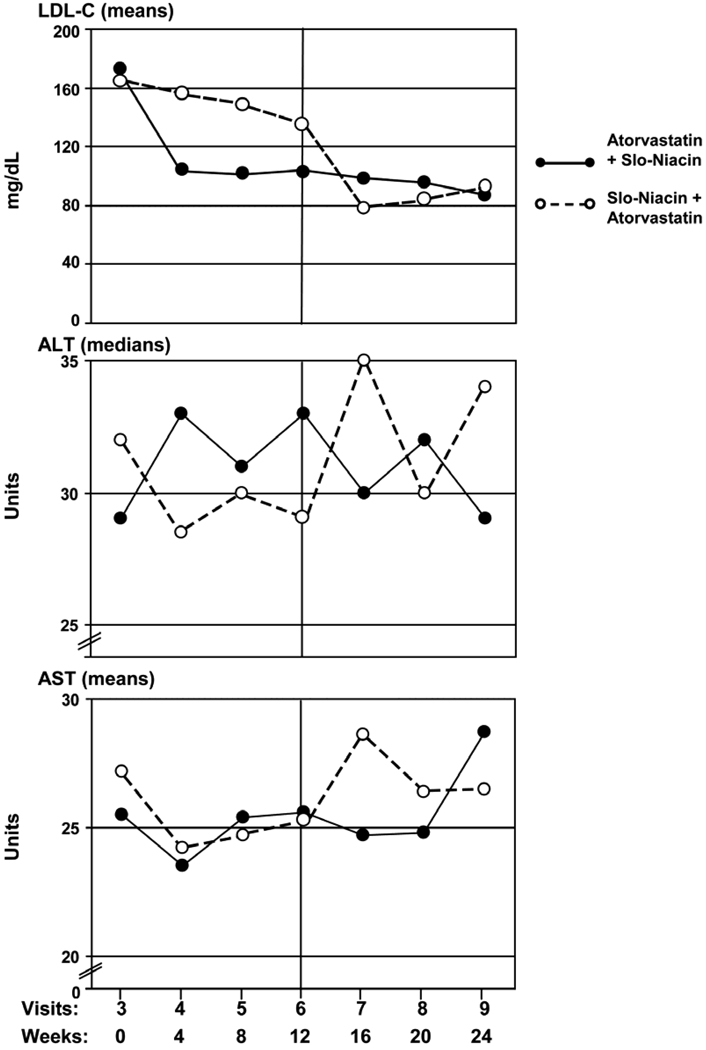
BACKGROUND: The combination of niacin and statin has proven value in hyperlipidemia management and heart disease prevention. However, the efficacy of the non-prescription time-release niacin, Slo-Niacin®, is little studied alone and not at all with atorvastatin. We gave Slo-Niacin® and atorvastatin, singly and together to determine efficacy on the combined abnormalities of triglyceride, LDL and HDL. METHODS: 42 men and women with LDL-C>130mg/dL HDL-C <45 (men or 55mg/dL (women) were randomized to 3 months of atorvastatin 10 mg/day or incremental doses of Slo-Niacin® to 1500 mg/day. The alternate drug was added in the next 3-month segment. Lipid profiles and transaminases were measured monthly and other measures at baseline and the end of each treatment sequence. RESULTS: Mean entry lipids (mg/dL) were: TG 187, LDL-C 171, and HDL-C 39. Mean BMI was 32.6 Kg/m(2). Monotherapy with Slo-Niacin® decreased median triglyceride 15%, mean LDL-C 12% and non-HDL-C 15% and increased HDL-C 8%. Atorvastatin decreased median triglyceride 26%, and mean LDL-C 36%, non-HDL-C 36% and increased HDL-C 6%. Combined therapy decreased median triglyceride 33% and mean LDL-C and non-HDL-C each 43%. HDL-C increased 10% (all p<0.001). Median remnant-like lipoprotein-C decreased 55%, mean apo-B 40%, median hsCRP 23% (all p<0.05), TNFa 12% and no change in IL-6. Mean LDL buoyancy increased 15%, apo-A-I 5% and median HDL(2)-C 20% (all p<0.05). ALT declined with Slo-Niacin® treatment alone compared to atorvastatin and also decreased when Slo-Niacin® was added to atorvastatin. Six subjects dropped out, 3 for niacin related symptoms. CONCLUSIONS: Slo-Niacin® 1.5g/day with atorvastatin 10 mg/day improved lipoprotein lipids, apoproteins and inflammation markers without hepatotoxicity. Slo-Niacin® deserves further study as a cost-effective treatment of hyperlipidemia.
Conflict of interest statement
Conflicts of interest: Dr. Knopp has served as a consultant to Upsher-Smith Laboratories, Inc. and as a consultant and speaker for Abbott Laboratories
Figures
References
-
- Knopp R, Paramsothy P, Atkinson B, Dowdy A. Comprehensive lipid management vs.aggressive LDL lowering to reduce cardiovascular risk. American Journal of Cardiology. 2008;101(suppl) 48B-57B. - PubMed
-
- Clofibrate and niacin in coronary heart disease. Jama. 1975;231:360–381. - PubMed
-
- Canner PL, Berge KG, Wenger NK, Stamler J, Friedman L, Prineas RJ, Friedewald W. Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. J Am Coll Cardiol. 1986;8:1245–1255. - PubMed
-
- Brown G, Albers JJ, Fisher LD, Schaefer SM, Lin JT, Kaplan C, Zhao XQ, Bisson BD, Fitzpatrick VF, Dodge HT. Regression of coronary artery disease as a result of intensive lipid-lowering therapy in men with high levels of apolipoprotein B. N Engl J Med. 1990;323:1289–1298. - PubMed
-
- Brown BG, Zhao XQ, Chait A, Fisher LD, Cheung MC, Morse JS, Dowdy AA, Marino EK, Bolson EL, Alaupovic P, Frohlich J, Albers JJ. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med. 2001;345:1583–1592. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous