

Case Reports
doi: 10.1186/1532-429X-12-1.
Cardiovascular magnetic resonance and PET-CT of left atrial paraganglioma
Affiliations
- PMID: 20047692
- PMCID: PMC2817869
- DOI: 10.1186/1532-429X-12-1
Item in Clipboard
Case Reports
Cardiovascular magnetic resonance and PET-CT of left atrial paraganglioma
J Cardiovasc Magn Reson.
.
Abstract
Cardiac paragangliomas are among the rarest primary cardiac tumors. We present a case of left atrial paraganglioma in a patient who presented with symptoms and signs of catecholamine excess in which cardiovascular magnetic resonance in multiple orientations and PET-CT played an important role in the diagnosis and tissue characterization.
Figures
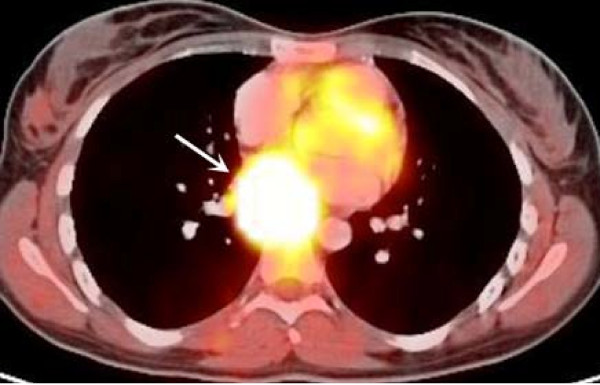
Axial view of PET-CT scan image demonstrates a large hypermetabolic mass with intense uptake of F18 Levo-DOPA in the posterior mediastinum near the left atrium which is consistent with paraganglioma.
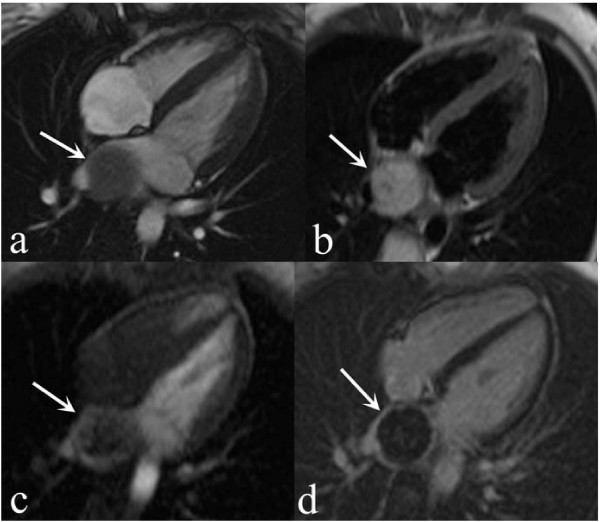
Horizontal long axis CMR images demonstrate a round, well defined posterior mediastinal mass with smooth extrinsic compression of left atrial wall which is hypo-intense on breath-hold Steady State Free Precession (SSFP) cine CMR (a, arrow), and shows homogenously high signal on T2-weighted dark blood turbo spin-echo image (b, arrow). T1-weighted inversion recovery gradient-echo myocardial perfusion imaging demonstrates heterogeneous, mostly peripheral, dynamic contrast filling of the mass suggesting vascularity (c, arrow), and T1-weighted, fat-saturated, inversion recovery late gadolinium enhancement image shows peripheral rim enhancement with no evidence of central enhancement suggestive of central tissue necrosis (d, arrow).
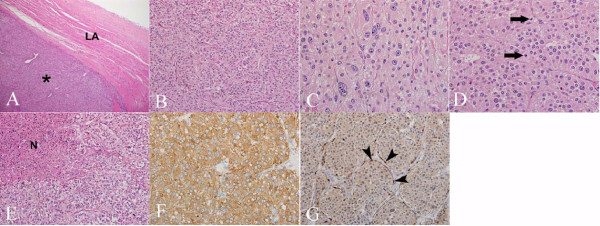
(A) Low power photomicrograph (40×; H&E stain) demonstrates tumor (*) compressing left atrium (LA). (B) The tumor is comprised of nests of fairly uniform cells with moderate eosinophilic, granular cytoplasm (200×; H&E stain). (C) Marked cytologic atypia with pleomorphic nuclei and prominent nucleoli was focally present (400×; H&E stain) in addition to (D) increased number of mitoses (arrows) (400×; H&E stain). (E) Scattered foci of coagulative tumor necrosis (N) were also noted (200×; H&E stain). (F) The tumor exhibited diffuse, strong cytoplasmic positivity for synaptophysin immunostain (400×). (G) S100 immunostain highlights sustentacular cells surrounding nests of tumor cells (400×).
