

Circumferential myocardial strain in cardiomyopathy with and without left bundle branch block
- PMID: 20047696
- PMCID: PMC2806866
- DOI: 10.1186/1532-429X-12-2
Circumferential myocardial strain in cardiomyopathy with and without left bundle branch block
Abstract
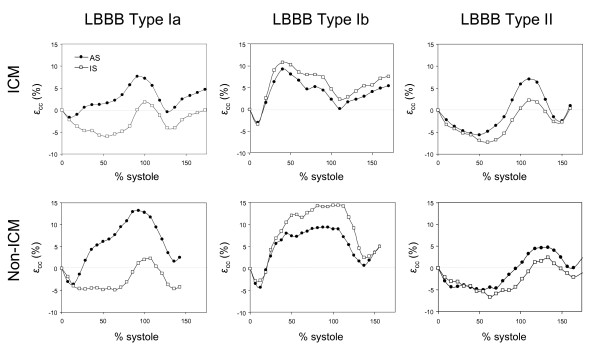
Background: Cardiac resynchronization therapy (CRT) has been shown to decrease mortality in 60-70% of advanced heart failure patients with left bundle branch block (LBBB) and QRS duration > 120 ms. There have been intense efforts to find reproducible non-invasive parameters to predict CRT response. We hypothesized that different left ventricular contraction patterns may exist in LBBB patients with depressed systolic function and applied tagged cardiovascular magnetic resonance (CMR) to assess circumferential strain in this population.
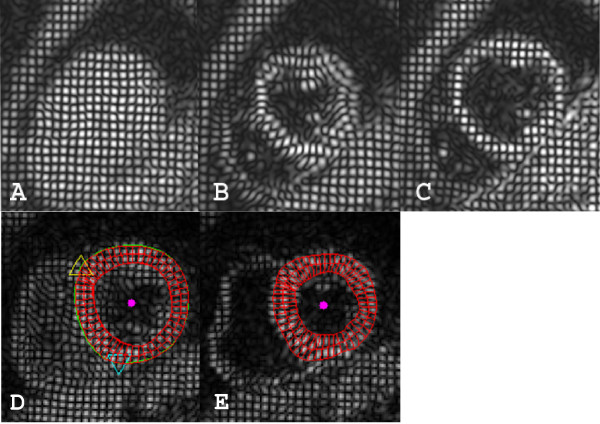
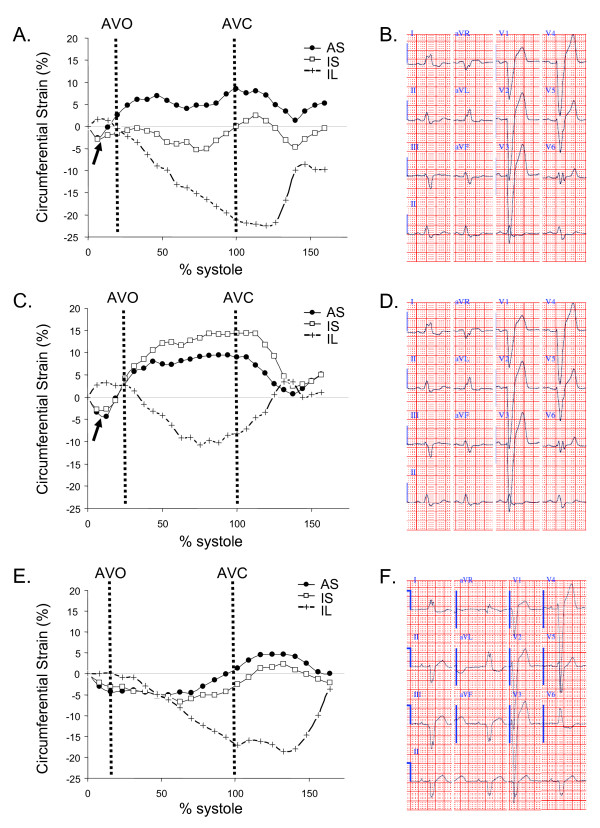
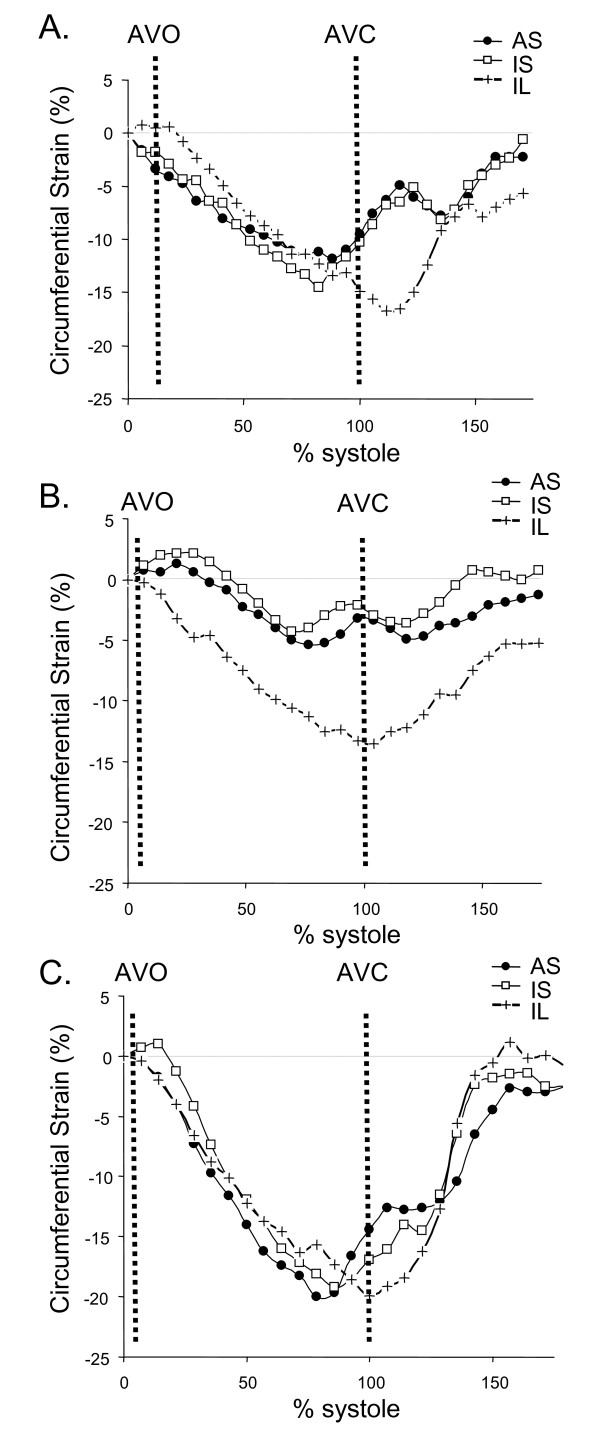
Methods: We determined myocardial circumferential strain at the basal, mid, and apical ventricular level in 35 subjects (10 with ischemic cardiomyopathy, 15 with non-ischemic cardiomyopathy, and 10 healthy controls). Patterns of circumferential strain were analyzed. Time to peak systolic circumferential strain in each of the 6 segments in all three ventricular slices and the standard deviation of time to peak strain in the basal and mid ventricular slices were determined.
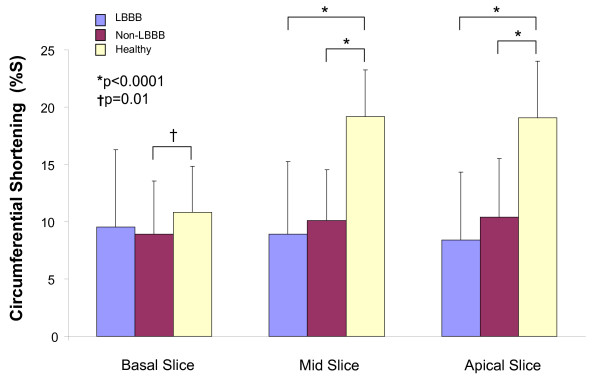
Results: Dyskinesis of the anterior septum and the inferior septum in at least two ventricular levels was seen in 50% (5 out of 10) of LBBB patients while 30% had isolated dyskinesis of the anteroseptum, and 20% had no dyskinesis in any segments, similar to all of the non-LBBB patients and healthy controls. Peak circumferential strain shortening was significantly reduced in all cardiomyopathy patients at the mid-ventricular level (LBBB 9 +/- 6%, non-LBBB 10 +/- 4% vs. healthy 19 +/- 4%; both p < 0.0001 compared to healthy), but was similar among the LBBB and non-LBBB groups (p = 0.20). The LBBB group had significantly greater dyssynchrony compared to the non-LBBB group and healthy controls assessed by opposing wall delays and 12-segment standard deviation (LBBB 164 +/- 30 ms vs. non-LBBB 70 +/- 17 ms (p < 0.0001), non-LBBB vs. healthy 65 +/- 17 ms (p = 0.47)).
Conclusions: Septal dyskinesis exists in some patients with LBBB. Myocardial circumferential strain analysis enables detailed characterization of contraction patterns, strengths, and timing in cardiomyopathy patients with and without LBBB.
Figures
References
-
- Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, Garrigue S, Kappenberger L, Haywood GA, Santini M, Bailleul C, Daubert JC. Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investigators. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001;344:873–880. doi: 10.1056/NEJM200103223441202. - DOI - PubMed
-
- Linde C, Abraham WT, Gold MR, St John Sutton M, Ghio S, Daubert C. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52:1834–1843. doi: 10.1016/j.jacc.2008.08.027. - DOI - PubMed
-
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL, Ellestad M, Trupp RJ, Underwood J, Pickering F, Truex C, McAtee P, Messenger J. MIRACLE Study Group. Multicenter InSync Randomized Clinical Evaluation. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002;346:1845–1853. doi: 10.1056/NEJMoa013168. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
