

Tumor and host factors that may limit efficacy of chemotherapy in non-small cell and small cell lung cancer
- PMID: 20047843
- PMCID: PMC2888634
- DOI: 10.1016/j.critrevonc.2009.11.006
Tumor and host factors that may limit efficacy of chemotherapy in non-small cell and small cell lung cancer
Abstract
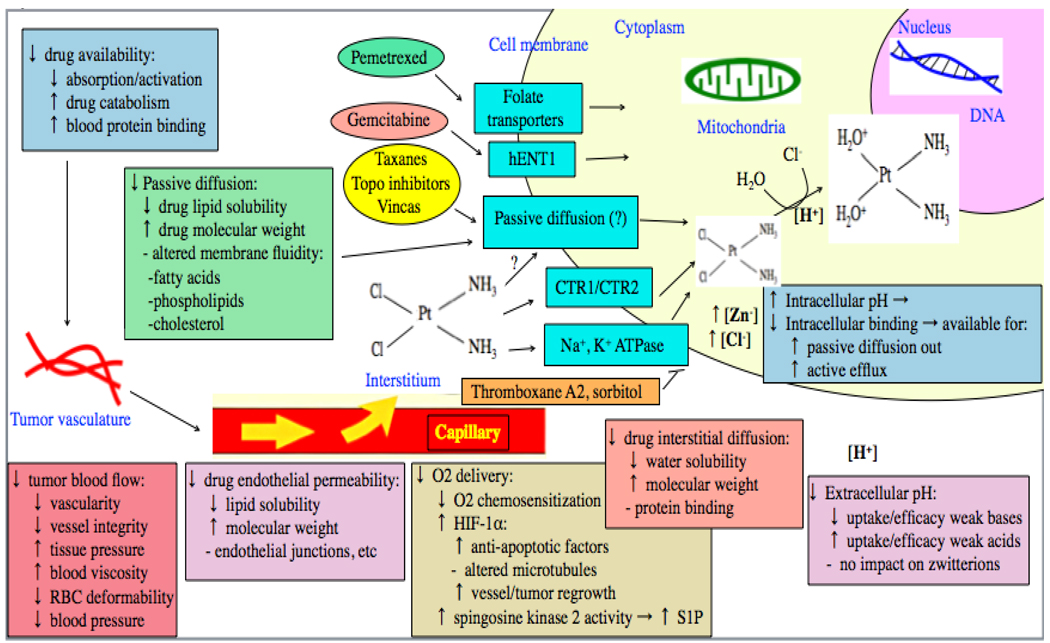
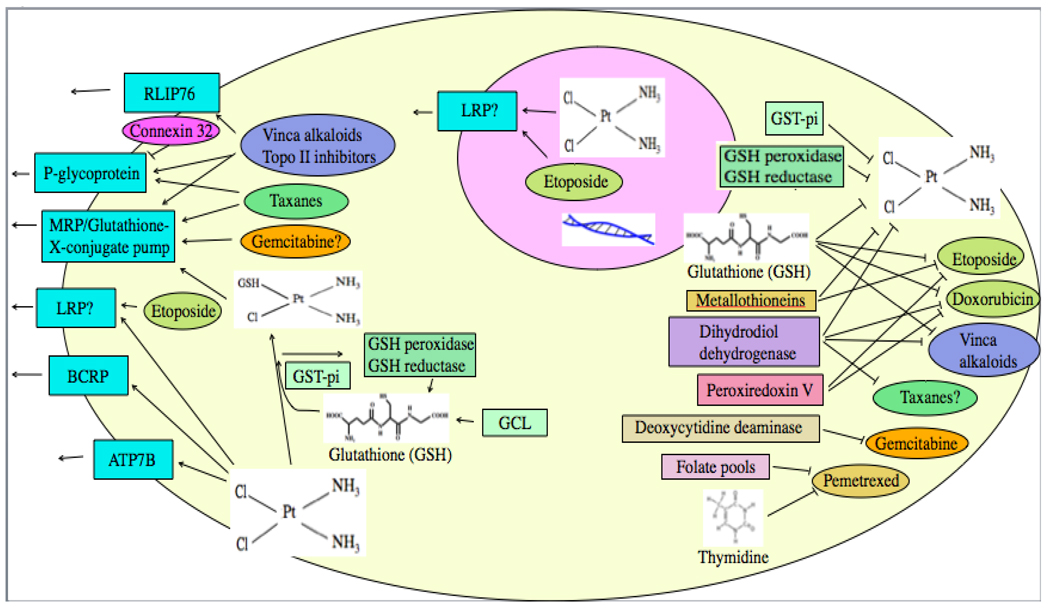
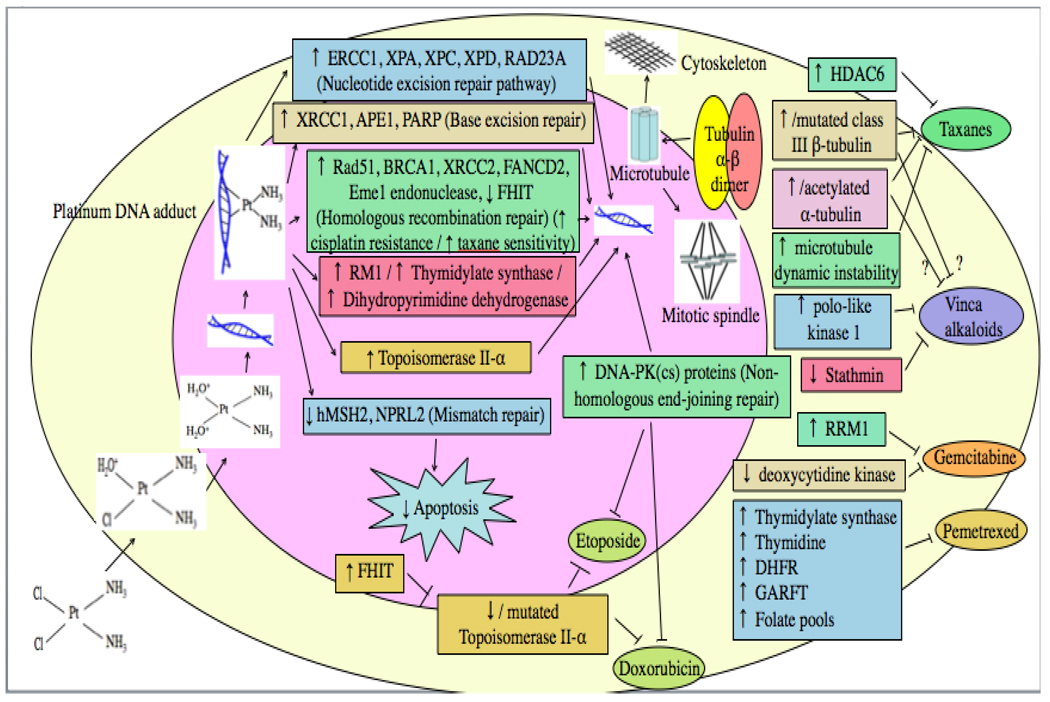
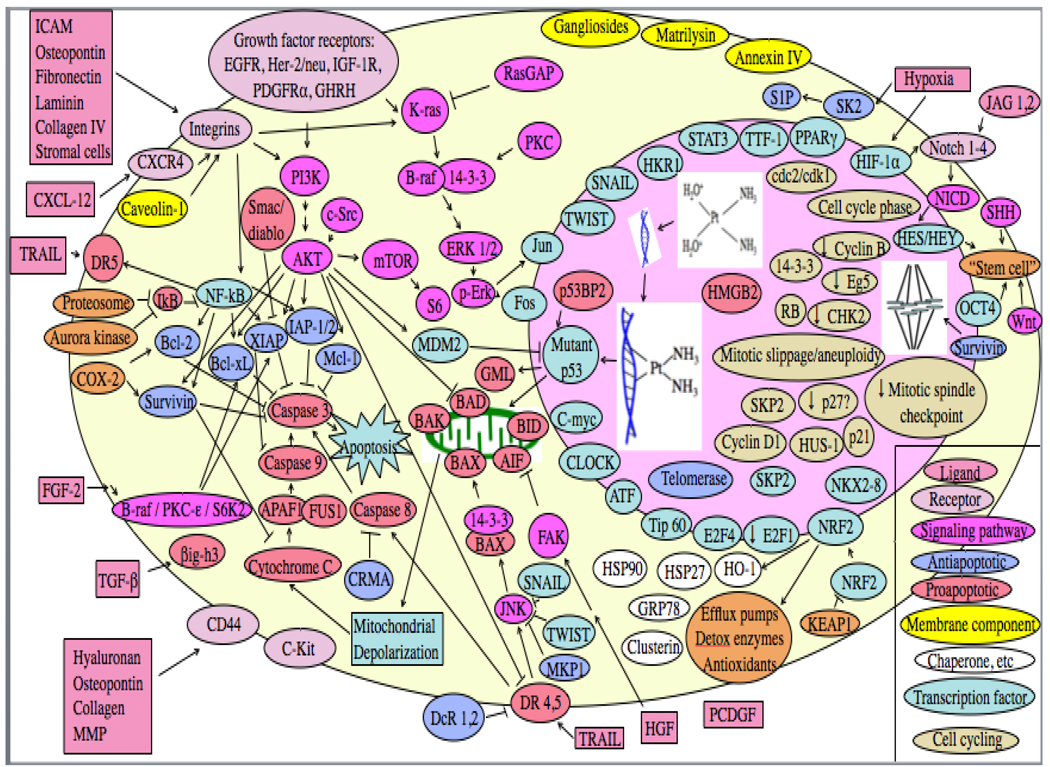
While chemotherapy provides useful palliation, advanced lung cancer remains incurable since those tumors that are initially sensitive to therapy rapidly develop acquired resistance. Resistance may arise from impaired drug delivery, extracellular factors, decreased drug uptake into tumor cells, increased drug efflux, drug inactivation by detoxifying factors, decreased drug activation or binding to target, altered target, increased damage repair, tolerance of damage, decreased proapoptotic factors, increased antiapoptotic factors, or altered cell cycling or transcription factors. Factors for which there is now substantial clinical evidence of a link to small cell lung cancer (SCLC) resistance to chemotherapy include MRP (for platinum-based combination chemotherapy) and MDR1/P-gp (for non-platinum agents). SPECT MIBI and Tc-TF scanning appears to predict chemotherapy benefit in SCLC. In non-small cell lung cancer (NSCLC), the strongest clinical evidence is for taxane resistance with elevated expression or mutation of class III beta-tubulin (and possibly alpha tubulin), platinum resistance and expression of ERCC1 or BCRP, gemcitabine resistance and RRM1 expression, and resistance to several agents and COX-2 expression (although COX-2 inhibitors have had minimal impact on drug efficacy clinically). Tumors expressing high BRCA1 may have increased resistance to platinums but increased sensitivity to taxanes. Limited early clinical data suggest that chemotherapy resistance in NSCLC may also be increased with decreased expression of cyclin B1 or of Eg5, or with increased expression of ICAM, matrilysin, osteopontin, DDH, survivin, PCDGF, caveolin-1, p21WAF1/CIP1, or 14-3-3sigma, and that IGF-1R inhibitors may increase efficacy of chemotherapy, particularly in squamous cell carcinomas. Equivocal data (with some positive studies but other negative studies) suggest that NSCLC tumors with some EGFR mutations may have increased sensitivity to chemotherapy, while K-ras mutations and expression of GST-pi, RB or p27kip1 may possibly confer resistance. While limited clinical data suggest that p53 mutations are associated with resistance to platinum-based therapies in NSCLC, data on p53 IHC positivity are equivocal. To date, resistance-modulating strategies have generally not proven clinically useful in lung cancer, although small randomized trials suggest a modest benefit of verapamil and related agents in NSCLC.
Published by Elsevier Ireland Ltd.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer Statistics, 2009. CA Cancer J Clin. 2009 - PubMed
-
- Stewart DJ, Tomiak E, Shamji FM, Maziak DE, MacLeod P, Phase II. study of alternating chemotherapy regimens for advanced non-small cell lung cancer. Lung Cancer. 2004;44:241–249. - PubMed
-
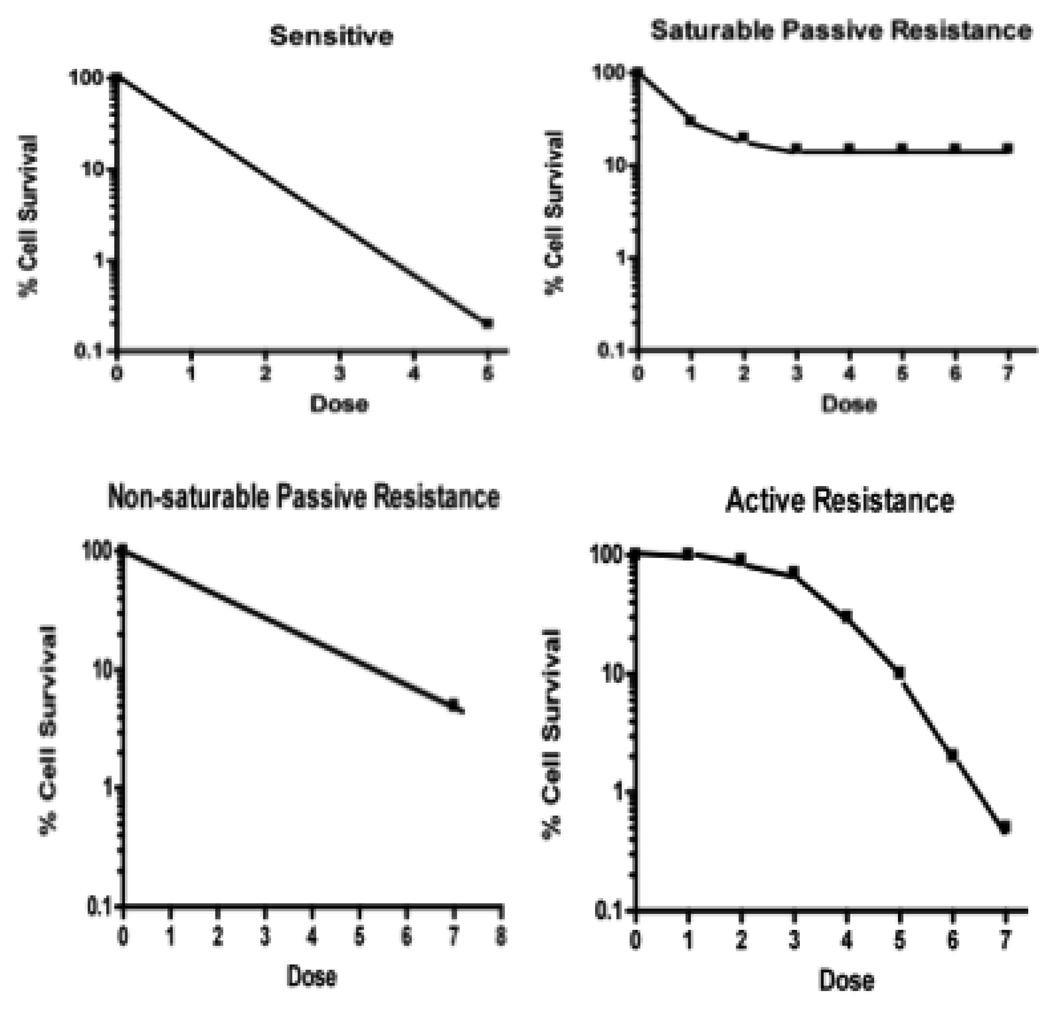
- Stewart DJ, Raaphorst GP, Yau J, Beaubien AR. Active vs. passive resistance, dose-response relationships, high dose chemotherapy, and resistance modulation: a hypothesis. Invest New Drugs. 1996;14:115–130. - PubMed
-
- Stewart DJ, Chiritescu G, Dahrouge S, Banerjee S, Tomiak EM. Chemotherapy dose--response relationships in non-small cell lung cancer and implied resistance mechanisms. Cancer Treat Rev. 2007;33:101–137. - PubMed
-
- Stordal B, Peters G, Davey R. Similar chromosomal changes in cisplatin and oxaliplatin-resistant sublines of the H69 SCLC cell line are not associated with platinum resistance. Genes Chromosomes Cancer. 2006;45:1094–1105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
