

The relationship between time to surgical debridement and incidence of infection after open high-energy lower extremity trauma
- PMID: 20048090
- PMCID: PMC2799040
- DOI: 10.2106/JBJS.H.00984
The relationship between time to surgical debridement and incidence of infection after open high-energy lower extremity trauma
Abstract
Background: Urgent débridement of open fractures has been considered to be of paramount importance for the prevention of infection. The purpose of the present study was to evaluate the relationship between the timing of the initial treatment of open fractures and the development of subsequent infection as well as to assess contributing factors.
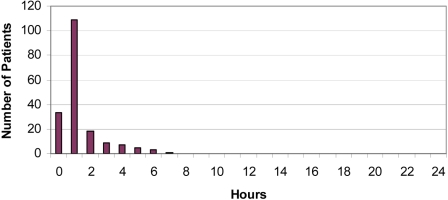
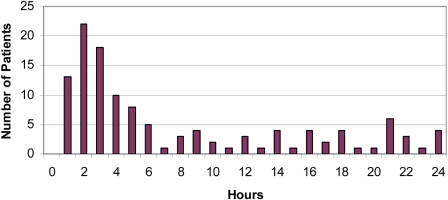
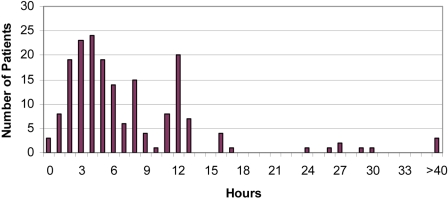
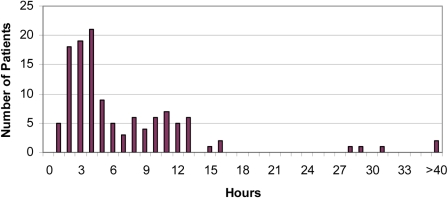
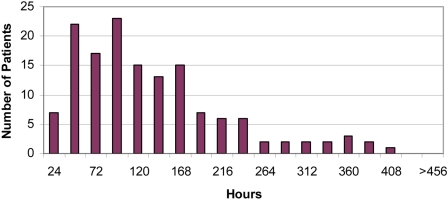
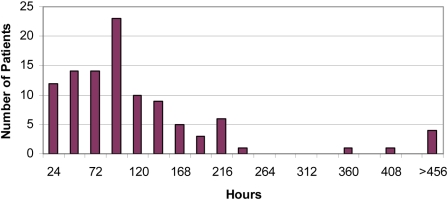
Methods: Three hundred and fifteen patients with severe high-energy lower extremity injuries were evaluated at eight level-I trauma centers. Treatment included aggressive débridement, antibiotic administration, fracture stabilization, and timely soft-tissue coverage. The times from injury to admission and operative débridement as well as a wide range of other patient, injury, and treatment-related characteristics that have been postulated to affect the risk of infection within the first three months after injury were studied, and differences between groups were calculated. In addition, multivariate logistic regression models were used to control for the effects of potentially confounding patient, injury, and treatment-related variables.
Results: Eighty-four patients (27%) had development of an infection within the first three months after the injury. No significant differences were found between patients who had development of an infection and those who did not when the groups were compared with regard to the time from the injury to the first débridement, the time from admission to the first débridement, or the time from the first débridement to soft-tissue coverage. The time between the injury and admission to the definitive trauma treatment center was an independent predictor of the likelihood of infection.
Conclusions: The time from the injury to operative débridement is not a significant independent predictor of the risk of infection. Timely admission to a definitive trauma treatment center has a significant beneficial influence on the incidence of infection after open high-energy lower extremity trauma.
Figures
References
-
- Pollak AN. Timing of débridement of open fractures. J Am Acad Orthop Surg. 2006;14(10 Spec No.):S48-51 - PubMed
-
- Werner CM, Pierpont Y, Pollak AN. The urgency of surgical debridement in the management of open fractures. J Am Acad Orthop Surg. 2008;16:369-75 - PubMed
-
- Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, Sanders RW, Jones AL, McAndrew MP, Patterson BM, McCarthy ML, Travison TG, Castillo RC. An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. N Engl J Med. 2002;347:1924-31 - PubMed
-
- MacKenzie EJ, Bosse MJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, Sanders RW, Jones AL, McAndrew MP, Patterson TM, McCarthy ML. Characterization of patients with high-energy lower extremity trauma. J Orthop Trauma. 2000;14:455-66 - PubMed
-
- MacKenzie EJ, Bosse MJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, Sanders R, Jones AL, McAndrew MP, Patterson B, McCarthy ML, Rohde CA, LEAP Study Group Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma. 2002;52:641-9 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
