

Validation of a web-based predictive nomogram for ipsilateral breast tumor recurrence after breast conserving therapy
- PMID: 20048188
- PMCID: PMC2834390
- DOI: 10.1200/JCO.2009.22.6662
Validation of a web-based predictive nomogram for ipsilateral breast tumor recurrence after breast conserving therapy
Abstract
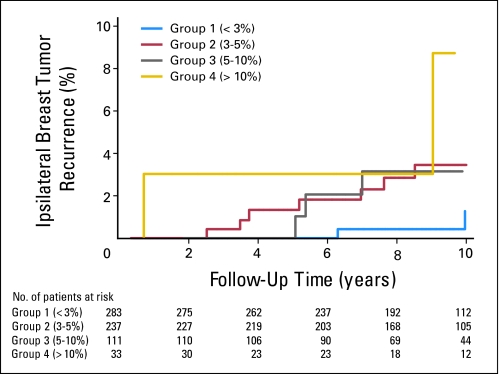
PURPOSE IBTR! version 1.0 is a web-based tool that uses literature-derived relative risk ratios for seven clinicopathologic variables to predict ipsilateral breast tumor recurrence (IBTR) after breast-conserving therapy (BCT). Preliminary testing demonstrated over-estimation in high-risk subgroups. This study uses two independent population-based datasets to create and validate a modified nomogram, IBTR! version 2.0. METHODS Cox regression modeling was performed on 7,811 patients treated with BCT at the British Columbia Cancer Agency (median follow-up, 9.4 years). Population-based hazard ratios were generated for the seven variables in the original nomogram. A modified nomogram was then tested against 664 patients from Massachusetts General Hospital (median follow-up, 9.3 years). The mean predicted and observed 10-year estimates were compared for the entire cohort and for four groups predefined by nomogram-predicted risks: group 1: less than 3%; group 2: 3% to 5%; group 3: 5% to 10%; and group 4: more than 10%. Results IBTR! version 2.0 predicted an overall 10-year IBTR estimate of 4.0% (95% CI, 3.8 to 4.2), while the observed estimate was 2.8% (95% CI, 1.6 to 4.7; P = .10). The predicted and observed IBTR estimates were: group 1 (n = 283): 2.2% versus 1.3%, P = .40; group 2 (n = 237): 3.8% versus 3.5%, P = .80; group 3 (n = 111): 6.7% versus 3.2%, P = .05; and group 4 (n = 33): 12.5% versus 8.7%, P = .50. CONCLUSION IBTR! version 2.0 is accurate in the majority of patients with a low to moderate risk of in-breast recurrence. The nomogram still overestimates risk in a minority of patients with higher risk features. Validation in a larger prospective data set is warranted.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Breast conservation treatment with radiation: an ongoing success story.J Clin Oncol. 2010 Feb 10;28(5):709-11. doi: 10.1200/JCO.2009.26.1164. Epub 2010 Jan 4. J Clin Oncol. 2010. PMID: 20048173 No abstract available.
Similar articles
-
Validation of the Web-Based IBTR! 2.0 Nomogram to Predict for Ipsilateral Breast Tumor Recurrence After Breast-Conserving Therapy.Int J Radiat Oncol Biol Phys. 2016 Aug 1;95(5):1477-1484. doi: 10.1016/j.ijrobp.2016.03.036. Epub 2016 Apr 2. Int J Radiat Oncol Biol Phys. 2016. PMID: 27315662
-
Validation of a nomogram in the prediction of local recurrence risks after conserving surgery for Asian women with ductal carcinoma in situ of the breast.Clin Oncol (R Coll Radiol). 2014 Nov;26(11):684-91. doi: 10.1016/j.clon.2014.08.004. Epub 2014 Sep 4. Clin Oncol (R Coll Radiol). 2014. PMID: 25194727
-
Validation of a Novel Nomogram for Prediction of Local Relapse after Surgery for Invasive Breast Carcinoma.Ann Surg Oncol. 2020 Jun;27(6):1864-1874. doi: 10.1245/s10434-019-08160-7. Epub 2020 Jan 21. Ann Surg Oncol. 2020. PMID: 31965372 Free PMC article.
-
Validation of a Web-Based Tool to Predict the Ipsilateral Breast Tumor Recurrence (IBTR! 2.0) after Breast-Conserving Therapy for Korean Patients.J Breast Cancer. 2013 Mar;16(1):97-103. doi: 10.4048/jbc.2013.16.1.97. Epub 2013 Mar 31. J Breast Cancer. 2013. PMID: 23593089 Free PMC article.
-
Repeat breast-conserving therapy for ipsilateral breast cancer recurrence: A systematic review.Eur J Surg Oncol. 2019 Aug;45(8):1317-1327. doi: 10.1016/j.ejso.2019.02.008. Epub 2019 Feb 10. Eur J Surg Oncol. 2019. PMID: 30795956
Cited by
-
Travel, Treatment Choice, and Survival Among Breast Cancer Patients: A Population-Based Analysis.Womens Health Rep (New Rochelle). 2021 Jan 11;2(1):1-10. doi: 10.1089/whr.2020.0094. eCollection 2021. Womens Health Rep (New Rochelle). 2021. PMID: 33786524 Free PMC article.
-
Magnetic resonance imaging-based prognostic model for subsequent distant metastasis in patients with ipsilateral breast tumor recurrence following breast-conserving surgery.Quant Imaging Med Surg. 2024 Jul 1;14(7):4506-4519. doi: 10.21037/qims-23-1831. Epub 2024 Jun 18. Quant Imaging Med Surg. 2024. PMID: 39022241 Free PMC article.
-
Local outcomes in ductal carcinoma in situ based on patient and tumor characteristics.J Natl Cancer Inst Monogr. 2010;2010(41):158-61. doi: 10.1093/jncimonographs/lgq031. J Natl Cancer Inst Monogr. 2010. PMID: 20956823 Free PMC article. Review.
-
Relationship between clinical features and distant metastases in rectal cancer predicted based on a nomogram: a retrospective cohort study.Sci Rep. 2024 Dec 28;14(1):31219. doi: 10.1038/s41598-024-82595-1. Sci Rep. 2024. PMID: 39732932 Free PMC article.
-
A comparison of a brachytherapy and an external beam radiotherapy boost in breast-conserving therapy for breast cancer: local and any recurrences.Strahlenther Onkol. 2019 Apr;195(4):310-317. doi: 10.1007/s00066-018-1413-0. Epub 2019 Jan 2. Strahlenther Onkol. 2019. PMID: 30603857 English.
References
-
- Early Breast Cancer Trialists' Collaborative Group. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;366:2087–2106. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–1241. - PubMed
-
- Veronesi U, Marubini E, Mariani L, et al. Radiotherapy after breast-conservation surgery in small breast carcinoma: Long-term results of a randomized trial. Ann Oncol. 2001;12:997–1003. - PubMed
-
- Clark R, Whelan T, Levine M, et al. Randomized clinical trial of breast irradiation following lumpectomy and axillary dissection for node negative breast cancer: An update. J Natl Cancer Inst. 1996;88:1659–1664. - PubMed
-
- Forrest A, Stewart H, Everington D, et al. Randomised controlled trial of conservation therapy for breast cancer: 6-year analysis of the Scottish trial. Scottish Cancer Trials Breast Group. Lancet. 1996;348:708–713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
