

Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension
- PMID: 20048214
- PMCID: PMC2846516
- DOI: 10.1161/CIRCULATIONAHA.108.844340
Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension
Abstract
Background: We tested the hypothesis that right ventricular (RV) pressure overload affects RV function and further influences left ventricular (LV) geometry, which adversely affects LV twist mechanics and segmental function.
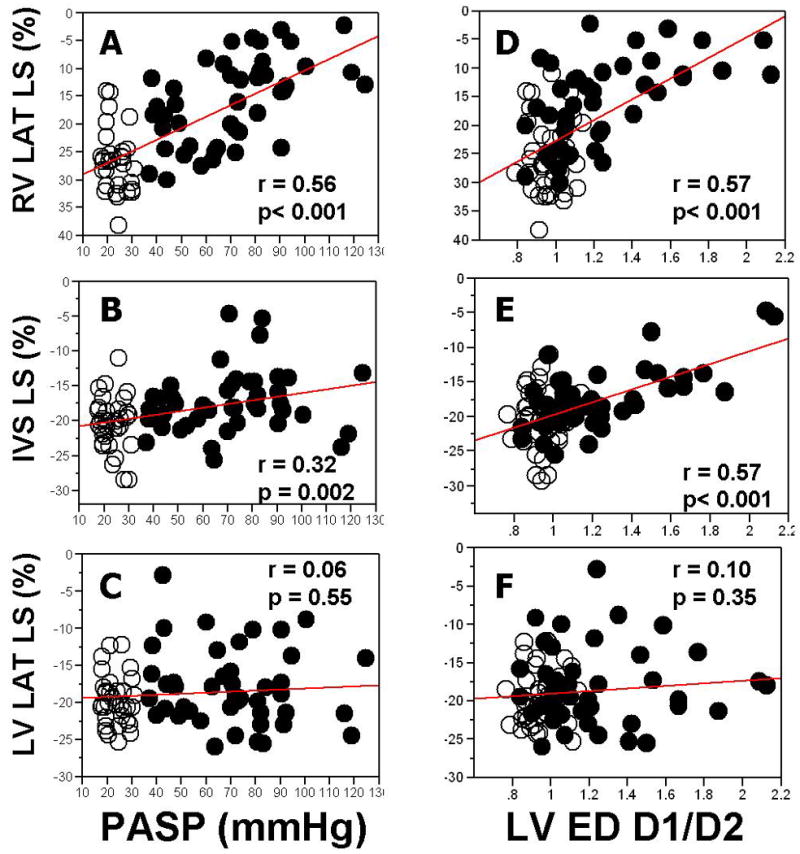
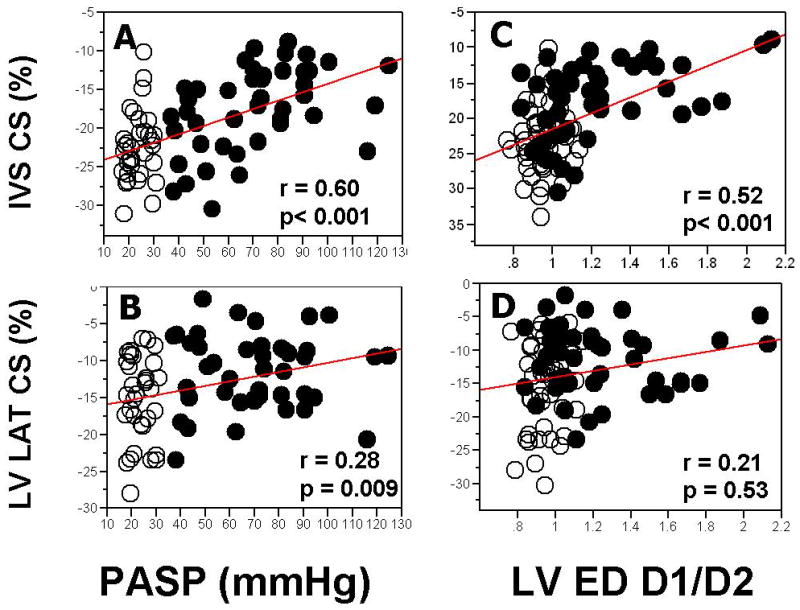
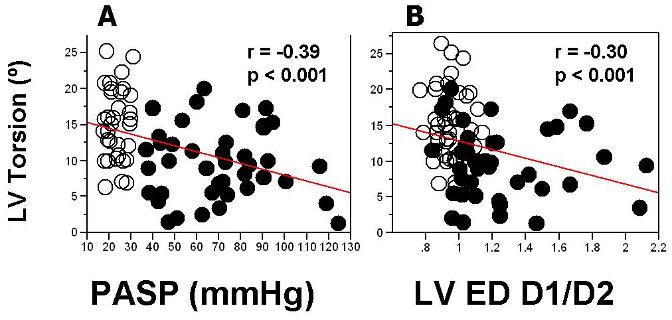
Methods and results: Echocardiographic images were prospectively acquired in 44 patients (age, 46+/-12 years; 82% women) with evidence of pulmonary hypertension (estimated pulmonary artery systolic pressure, 71+/-23 mm Hg) and in 44 age- and gender-matched healthy subjects. Patients with intrinsic LV diseases were excluded. RV lateral wall longitudinal strain (LS) and interventricular septal (IVS) LS were reduced in the pulmonary hypertension group compared with control subjects (-15.9+/-7.6% versus -25.5+/-6.1%, P<0.001; and -17.3+/-4.4% versus -20.2+/-3.9%, P=0.002, respectively), whereas LV lateral wall LS was preserved. RV lateral wall LS and IVS LS, but not LV lateral wall LS, correlated with pulmonary artery systolic pressure (r=0.56, P<0.01; r=0.32, P<0.01) and LV eccentricity index (r=0.57, P<0.01; r=0.57, P<0.01). IVS and LV lateral wall circumferential strain (CS) were both reduced in the pulmonary hypertension group. Although IVS CS and LV lateral wall CS correlated with pulmonary artery systolic pressure and LV eccentricity index, after adjustment of CS for LV eccentricity index, differences between groups persisted for IVS CS (P<0.01) but not LV lateral wall CS (P=0.09). LV torsion was decreased in patients with pulmonary hypertension compared with control subjects (9.6+/-4.9 degrees versus 14.7+/-4.9 degrees , P<0.001). LV torsion inversely correlated with pulmonary artery systolic pressure (r=-0.39, P<0.01) and LV eccentricity index (r=-0.3, P<0.01). LV untwisting rates were similar in both groups (P=0.7).
Conclusions: Chronic RV pressure overload directly affects RV longitudinal systolic deformation. RV pressure overload further influences IVS and LV geometry, which impairs LV torsion and segmental LS and CS, more for the IVS than for the free wall of the LV.
Conflict of interest statement
Figures
References
-
- Moon MR, Bolger AF, DeAnda A, Komeda M, Daughters GT, 2nd, Nikolic SD, Miller DC, Ingels NB., Jr Septal function during left ventricular unloading. Circulation. 1997;95:1320–7. - PubMed
-
- Raymond RJ, Hinderliter AL, Willis PW, Ralph D, Caldwell EJ, Williams W, Ettinger NA, Hill NS, Summer WR, de Boisblanc B, Schwartz T, Koch G, Clayton LM, Jobsis MM, Crow JW, Long W. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol. 2002;39:1214–9. - PubMed
-
- Simonneau G, Galie N, Rubin LJ, Langleben D, Seeger W, Domenighetti G, Gibbs S, Lebrec D, Speich R, Beghetti M, Rich S, Fishman A. Clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2004;43:5S–12S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
