

Complications and monitoring - Guidelines on Parenteral Nutrition, Chapter 11
- PMID: 20049074
- PMCID: PMC2795374
- DOI: 10.3205/000076
Complications and monitoring - Guidelines on Parenteral Nutrition, Chapter 11
Abstract
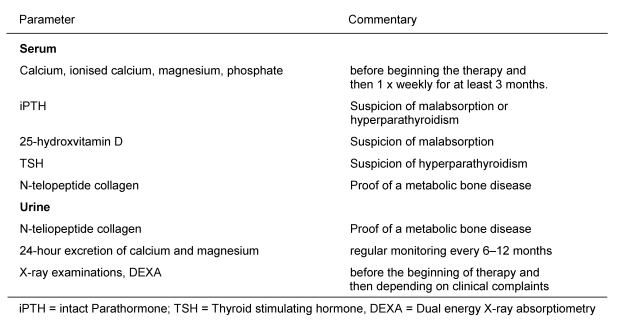
Compared to enteral or hypocaloric oral nutrition, the use of PN (parenteral nutrition) is not associated with increased mortality, overall frequency of complications, or longer length of hospital stay (LOS). The risk of PN complications (e.g. refeeding-syndrome, hyperglycaemia, bone demineralisation, catheter infections) can be minimised by carefully monitoring patients and the use of nutrition support teams particularly during long-term PN. Occuring complications are e.g. the refeeding-syndrome in patients suffering from severe malnutrition with the initiation of refeeding or metabolic, hypertriglyceridemia, hyperglycaemia, osteomalacia and osteoporosis, and hepatic complications including fatty liver, non-alcoholic fatty liver disease, cholestasis, cholecystitis, and cholelithiasis. Efficient monitoring in all types of PN can result in reduced PN-associated complications and reduced costs. Water and electrolyte balance, blood sugar, and cardiovascular function should regularly be monitored during PN. Regular checks of serum electrolytes and triglycerides as well as additional monitoring measures are necessary in patients with altered renal function, electrolyte-free substrate intake, lipid infusions, and in intensive care patients. The metabolic monitoring of patients under long-term PN should be carried out according to standardised procedures. Monitoring metabolic determinants of bone metabolism is particularly important in patients receiving long-term PN. Markers of intermediary, electrolyte and trace element metabolism require regular checks.
Im Vergleich zu einer enteralen bzw. hypokalorisch oralen Ernährung ist die PE (parenterale Ernährung) nicht mit einer erhöhten Letalität, Komplikationshäufigkeit insgesamt und Krankenhausverweildauer verbunden. Das Risiko durch PE verursachter Komplikationen (wie z.B. Refeeding-Syndrom, Hyperglykämie, Knochendemineralisierung, Katheterinfektionen) kann durch eine sorgfältige Überwachung des Patienten und durch den Einsatz von Ernährungsteams, besonders während einer Langzeit-PE, minimiert werden. Auftretende Komplikationen sind z.B. das Refeeding-Syndrom bei Patienten mit ausgeprägter Mangelernährung, bei denen eine erneute Ernährung begonnen wird. Weitere schwere Nebenwirkungen können metabolische und hepatische Komplikationen sein, wie eine Hypertriglyzeridämie, Hyperglykämie, Fettleber, Steatohepatitis, Cholestase, Cholezystitis, Cholelithiasis sowie Osteomalazie und Osteoporose. Die Effizienzkontrolle bei jeder Art von PE kann zur Reduktion von PE-assoziierten Komplikationen und zur Kostensenkung führen. Unter PE sollte Wasser,- Elektrolyt- und Zuckerhaushalt sowie die kardiozirkuläre Funktion engmaschig überwacht werden. Regelmäßige Kontrollen der Serumelektrolyte und der Triglyzeride sind unter PE erforderlich sowie zusätzliche Überwachungsmaßnahmen bei Patienten mit Nierenfunktionsstörungen, bei elektrolytfreier Substratzufuhr, Fettinfusion bzw. bei Intensivpatienten. Das metabolische Monitoring von Patienten unter längerfristiger PE sollte nach standardisierten Schemata erfolgen. Unter Langzeit-PE sind zusätzlich die metabolischen Determinanten des Knochenstoffwechsels überwachungspflichtig. Variablen des Intermediär-, Elektrolyt- und Spurenelementstoffwechsels bedürfen einer Kontrolle in regelmäßigen Abständen.
Keywords: catheter infection; hyperglycaemia; hypertriglyceridemia; liver disease; refeeding syndrome.
Figures
References
-
- ASPEN Board of Directors and the Clinical Guidelines Task Force. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN J Parenter Enteral Nutr. 2002;26(1 Suppl):1SA–138SA. - PubMed
-
- Maroulis J, Kalfarentzos F. Complications of parenteral nutrition at the end of the century. Clin Nutr. 2000;19:295–304. doi: 10.1054/clnu.1999.0089. Available from: http://dx.doi.org/10.1054/clnu.1999.0089. - DOI - DOI - PubMed
-
- Koretz RL, Lipman TO, Klein S American Gastroenterological Association. AGA technical review on parenteral nutrition. Gastroenterology. 2001;121(4):970–1001. doi: 10.1016/S0016-5085(01)92000-1. Available from: http://dx.doi.org/10.1016/S0016-5085(01)92000-1. - DOI - DOI - PubMed
-
- Braunschweig CL, Levy P, Sheean PM, Wang X. Enteral compared with parenteral nutrition: a meta-analysis. Am J Clin Nutr. 2001;74(4):534–542. - PubMed
-
- Van den Berghe G. Insulin therapy for the critically ill patient. Clin Cornerstone. 2003;5(2):56–63. doi: 10.1016/S1098-3597(03)90018-4. Available from: http://dx.doi.org/10.1016/S1098-3597(03)90018-4. - DOI - DOI - PubMed
