

Access technique and its problems in parenteral nutrition - Guidelines on Parenteral Nutrition, Chapter 9
- PMID: 20049083
- PMCID: PMC2795383
- DOI: 10.3205/000078
Access technique and its problems in parenteral nutrition - Guidelines on Parenteral Nutrition, Chapter 9
Abstract
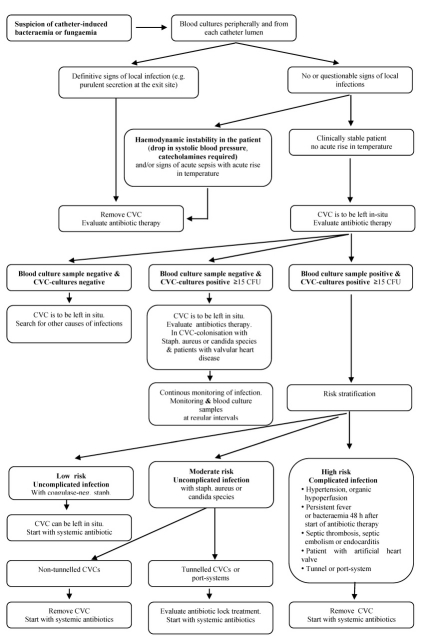
Catheter type, access technique, and the catheter position should be selected considering to the anticipated duration of PN aiming at the lowest complication risks (infectious and non-infectious). Long-term (>7-10 days) parenteral nutrition (PN) requires central venous access whereas for PN <3 weeks percutaneously inserted catheters and for PN >3 weeks subcutaneous tunnelled catheters or port systems are appropriate. CVC (central venous catheter) should be flushed with isotonic NaCl solution before and after PN application and during CVC occlusions. Strict indications are required for central venous access placement and the catheter should be removed as soon as possible if not required any more. Blood samples should not to be taken from the CVC. If catheter infection is suspected, peripheral blood-culture samples and culture samples from each catheter lumen should be taken simultaneously. Removal of the CVC should be carried out immediately if there are pronounced signs of local infection at the insertion site and/or clinical suspicion of catheter-induced sepsis. In case PN is indicated for a short period (max. 7-10 days), a peripheral venous access can be used if no hyperosmolar solutions (>800 mosm/L) or solutions with a high titration acidity or alkalinity are used. A peripheral venous catheter (PVC) can remain in situ for as long as it is clinically required unless there are signs of inflammation at the insertion site.
Abhängig von der voraussichtlichen Dauer der PE sollte der Kathetertyp, die Zugangstechnik und die Katheterposition mit dem geringsten Komplikationsrisiko (infektiös und nicht-infektiös) gewählt werden. Eine langfristige (>7–10 Tage), bedarfsadaptierte parenterale Ernährung (PE) ist auf einen suffizienten zentralvenösen Zugangsweg angewiesen, wobei für eine PE <3 Wochen perkutan eingelegte Katheter und für eine PE >3 Wochen subkutan tunnelierte Katheter oder implantierte Portsysteme zur Anwendung kommen. Der zentralvenöse Katheter (ZVK) sollte vor und nach der PE-Applikation und bei ZVK-Okklusion mit physiologischer NaCl-Lösung gespült werden. Die Indikationsstellung zur Anlage eines venösen Zugangs muss streng erfolgen und der Katheter sollte schnellst möglich wieder entfernt werden, wenn er nicht mehr benötigt wird. Zur Reduktion des Infektionsrisikos sollten Blutentnahmen aus dem ZVK vermieden werden. Bei Verdacht auf Katheterinfektion sollten gleichzeitig Blutkulturen peripher und aus jedem Katheterlumen entnommen werden. Bei ausgeprägten lokalen Infektzeichen der Insertionsstelle und klinischem Verdacht auf Katheter-induzierte Blutstrom-Infektion ist die ZVK-Neuanlage vorzunehmen. Im Falle einer kurzzeitig indizierten PE (max. 7–10 Tage) kann eine periphervenöse Zufuhr durchgeführt werden, wenn keine hyperosmolaren Lösungen (>800 mosm/l) und keine Lösungen mit einer hohen Titrationsazidität bzw. -alkalität (Bikarbonat, Trispuffer) appliziert werden. Die periphere Kanüle (PVK) kann so lange liegen bleiben, wie sie benötigt wird, wenn an der Einstichstelle keine Entzündungszeichen auftreten.
Keywords: catheter-related infections; central venous catheter; handling of central catheter; in-line filter; intravenous access.
Figures
References
-
- Krzywda EA, Andris DA, Edmiston CE. Catheter infections: Diagnosis, etiology, treatment and prevention. Nutr Clin Pract. 1999;14:178. doi: 10.1177/088453369901400405. Available from: http://dx.doi.org/10.1177/088453369901400405. - DOI - DOI
-
- Chung DH, Ziegler MM. Central venous catheter access. Nutrition. 1998;14:119–123. doi: 10.1016/S0899-9007(97)00228-1. Available from: http://dx.doi.org/10.1016/S0899-9007(97)00228-1. - DOI - DOI - PubMed
-
- Meadows N. Monitoring and complications of parenteral nutrition. Nutrition. 1998;14:806–808. doi: 10.1016/S0899-9007(98)00089-6. Available from: http://dx.doi.org/10.1016/S0899-9007(98)00089-6. - DOI - DOI - PubMed
-
- Lederle FA, Parenti CM, Berskow LC, Ellingson KJ. The idle intravenous catheter. Ann Intern Med. 1992;116(9):737–738. - PubMed
-
- Parenti CM, Lederle FA, Impola CL, Peterson LR. Reduction of unnecessary intravenous catheter use; Internal medicine house staff participate in a successful quality improvement project. Arch Intern Med. 1994;154(16):1829–1832. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
