

Cerebrospinal fluid tau and ptau(181) increase with cortical amyloid deposition in cognitively normal individuals: implications for future clinical trials of Alzheimer's disease
- PMID: 20049742
- PMCID: PMC2806678
- DOI: 10.1002/emmm.200900048
Cerebrospinal fluid tau and ptau(181) increase with cortical amyloid deposition in cognitively normal individuals: implications for future clinical trials of Alzheimer's disease
Abstract
Alzheimer's disease (AD) pathology is estimated to develop many years before detectable cognitive decline. Fluid and imaging biomarkers may identify people in early symptomatic and even preclinical stages, possibly when potential treatments can best preserve cognitive function. We previously reported that cerebrospinal fluid (CSF) levels of amyloid-beta(42) (Abeta(42)) serve as an excellent marker for brain amyloid as detected by the amyloid tracer, Pittsburgh compound B (PIB). Using data from 189 cognitively normal participants, we now report a positive linear relationship between CSF tau/ptau(181) (primary constituents of neurofibrillary tangles) with the amount of cortical amyloid. We observe a strong inverse relationship of cortical PIB binding with CSF Abeta(42) but not for plasma Abeta species. Some individuals have low CSF Abeta(42) but no cortical PIB binding. Together, these data suggest that changes in brain Abeta(42) metabolism and amyloid formation are early pathogenic events in AD, and that significant disruptions in CSF tau metabolism likely occur after Abeta(42) initially aggregates and increases as amyloid accumulates. These findings have important implications for preclinical AD diagnosis and treatment.
Figures
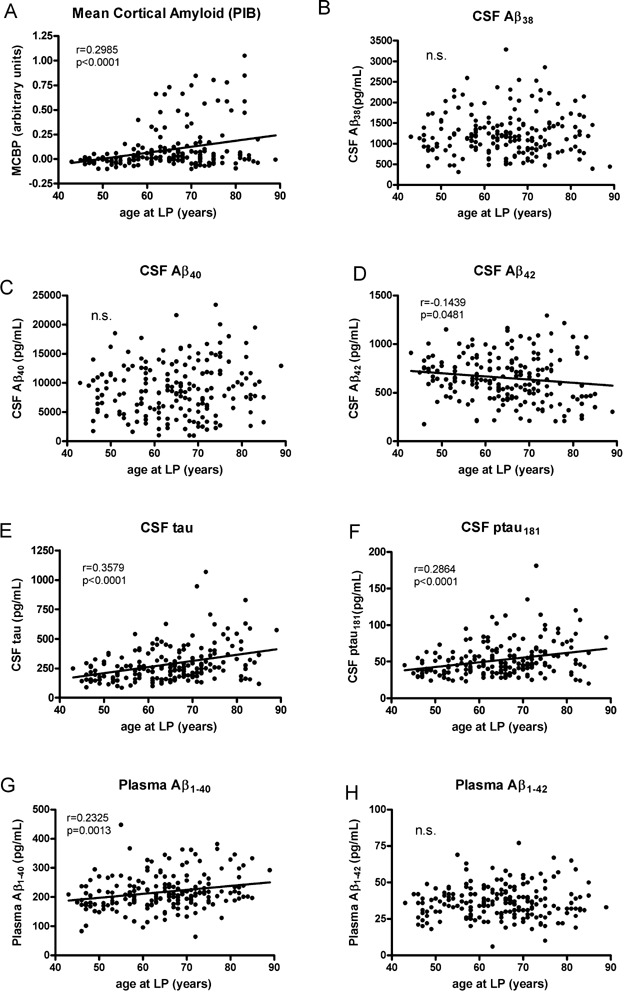
cortical amyloid are positively correlated with age in this CDR 0 cohort,
The level of CSF Aβ38 is not correlated with age,
nor is CSF Aβ40.
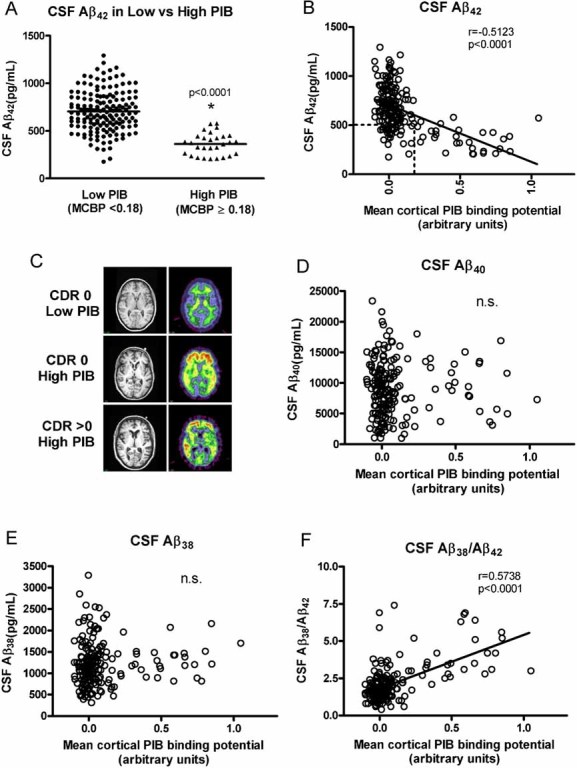
CSF Aβ42 is negatively correlated with age.
Positive correlations with age are observed for CSF tau,
CSF ptau181 and
plasma Aβ1–40.
Plasma Aβ1–42 is not correlated with age in this cohort.
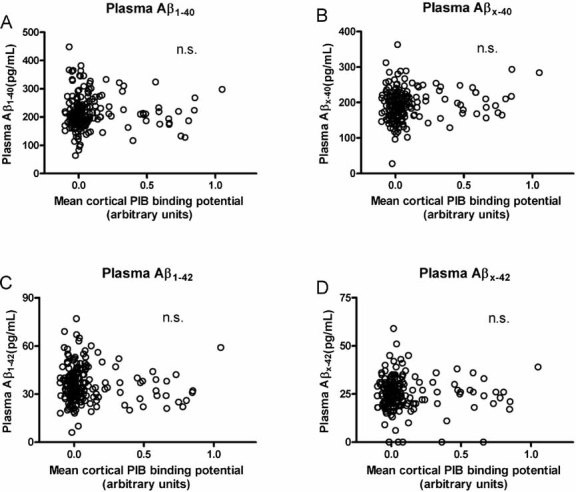
Aβ1–40 (r = −0.0724, p = 0.3234),
Aβx–40 (r = 0.04583, p = 0.5323),
Aβ1–42 (r = −0.1015, p = 0.1658) or
Aβx–42 (r = −0.03869, p = 0.5981). Five participants had levels of plasma Aβx–42 below the level of detection so they are represented as having 0 pg/ml. All Pearson correlation coefficients are corrected for age. n.s., not significant.
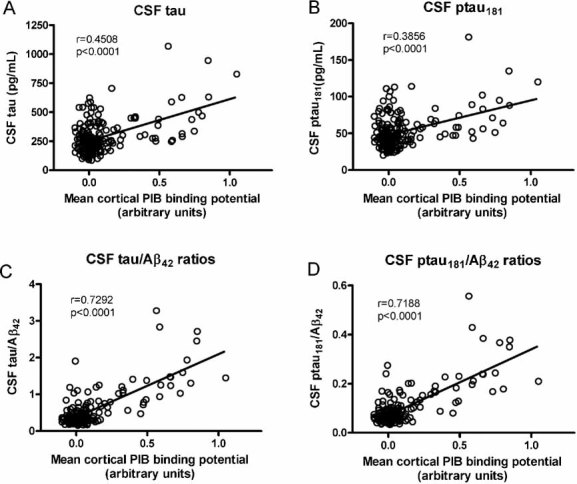
the levels of CSF tau
the levels of CSF ptau181
the ratios of CSF tau/Aβ42 and
the ratios of the ptau181/Aβ42. The correlations between the CSF tau(s)/Aβ42 ratios and MCBP remain significant even when the statistical outlier (high PIB, high ratio) is omitted from the analysis (tau/Aβ42, r = 0.74227, p < 0.0001; ptau181/Aβ42, r = 0.73510, p < 0.0001). All Pearson correlation coefficients are corrected for age.
References
-
- Armitage S. An analysis of certain psychological tests used in the evaluation of brain injury. Psych Mono. 1946;60:1–48.
-
- Berg L, McKeel DW, Miller JP, Storandt M, Rubin EH, Morris JC, Baty J, Coats M, Norton J, Goate AM, et al. Clinicopathologic studies in cognitively healthy aging and Alzheimer's disease—relation of histologic markers to dementia severity, age, sex, and apoE genotype. Arch Neurol. 1998;55:326–335. - PubMed
-
- Blennow K, Meyer GD, Hansson O, Minthon L, Wallin A, Zetterberg H, Lewczuk P, Vanderstichele H, Vanmechelen E, Kornhuber J, et al. Evolution of Abeta42 and Abeta40 Levels and Abeta42/Abeta40 ratio in plasma during progression of Alzheimer's disease: a multicenter assessment. J Nutr Health Aging. 2009;13:205–208. - PubMed
