

Do all psychological treatments really work the same in posttraumatic stress disorder?
- PMID: 20051310
- PMCID: PMC2852651
- DOI: 10.1016/j.cpr.2009.12.001
Do all psychological treatments really work the same in posttraumatic stress disorder?
Abstract
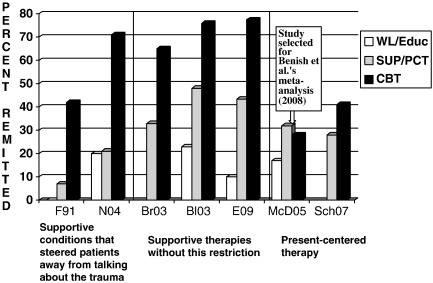
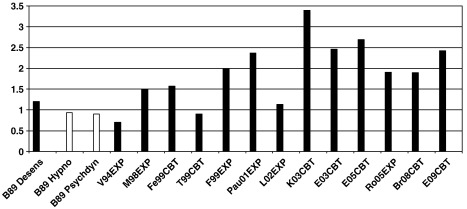
A recent meta-analysis by Benish, Imel, and Wampold (2008, Clinical Psychology Review, 28, 746-758) concluded that all bona fide treatments are equally effective in posttraumatic stress disorder (PTSD). In contrast, seven other meta-analyses or systematic reviews concluded that there is good evidence that trauma-focused psychological treatments (trauma-focused cognitive behavior therapy and eye movement desensitization and reprocessing) are effective in PTSD; but that treatments that do not focus on the patients' trauma memories or their meanings are either less effective or not yet sufficiently studied. International treatment guidelines therefore recommend trauma-focused psychological treatments as first-line treatments for PTSD. We examine possible reasons for the discrepant conclusions and argue that (1) the selection procedure of the available evidence used in Benish et al.'s (2008)meta-analysis introduces bias, and (2) the analysis and conclusions fail to take into account the need to demonstrate that treatments for PTSD are more effective than natural recovery. Furthermore, significant increases in effect sizes of trauma-focused cognitive behavior therapies over the past two decades contradict the conclusion that content of treatment does not matter. To advance understanding of the optimal treatment for PTSD, we recommend further research into the active mechanisms of therapeutic change, including treatment elements commonly considered to be non-specific. We also recommend transparency in reporting exclusions in meta-analyses and suggest that bona fide treatments should be defined on empirical and theoretical grounds rather than by judgments of the investigators' intent.
Copyright 2009 Elsevier Ltd. All rights reserved.
Figures
References
-
- American Psychiatric Association (2004). Treatment of patients with acute stress disorder and posttraumatic stress disorder. http://www.psychiatryonline.com/pracGuide/pracGuideTopic_11.aspx. - PubMed
-
- Australian Centre for Posttraumatic Mental Health (2007). Australian guidelines for the treatment of adults with acute stress disorder and posttraumatic stress disorder. http://www.acpmh.unimelb.edu.au.
-
- Benish S.G., Imel Z.E., Wampold B.E. The relative efficacy of bona fide psychotherapies for treating post-traumatic stress disorder: A meta-analysis of direct comparisons. Clinical Psychology Review. 2008;28:746–758. - PubMed
-
- Bisson, J., & Andrew, M. (2009). Psychological treatments of post-traumatic stress disorder (PTSD) (Review). The Cochrane Library, 2009 (2), http://www.thecochranelibrary.com. - PubMed
-
- Bisson J., Ehlers A., Matthews R., Pilling S., Richards D., Turner S. Systematic review and metaanalysis of psychological treatments for posttraumatic stress disorder. British Journal of Psychiatry. 2007;190:97–104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
