

Expanding role of 18F-fluoro-D-deoxyglucose PET and PET/CT in spinal infections
- PMID: 20052505
- PMCID: PMC2899827
- DOI: 10.1007/s00586-009-1251-y
Expanding role of 18F-fluoro-D-deoxyglucose PET and PET/CT in spinal infections
Abstract
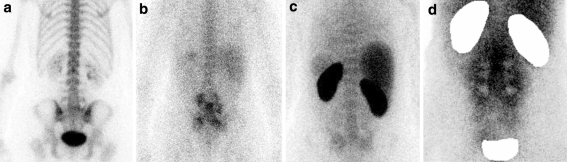
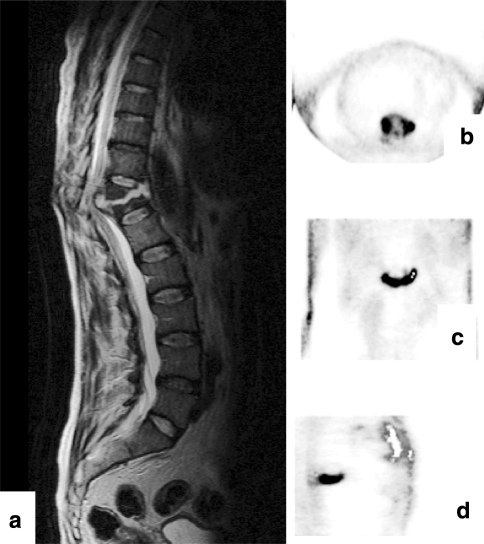
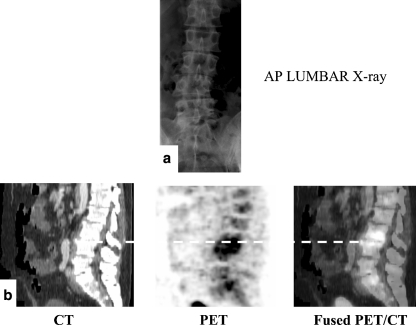
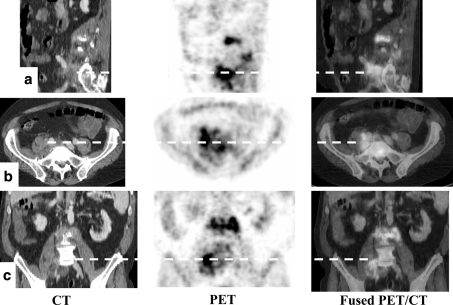
(18)F-fluoro-D -deoxyglucose positron emission tomography ([(18)F]-FDG PET) is successfully employed as a molecular imaging technique in oncology, and has become a promising imaging modality in the field of infection. The non-invasive diagnosis of spinal infections (SI) has been a challenge for physicians for many years. Morphological imaging modalities such as conventional radiography, computed tomography (CT), and magnetic resonance imaging (MRI) are techniques frequently used in patients with SI. However, these methods are sometimes non-specific, and difficulties in differentiating infectious from degenerative end-plate abnormalities or postoperative changes can occur. Moreover, in contrast to CT and MRI, FDG uptake in PET is not hampered by metallic implant-associated artifacts. Conventional radionuclide imaging tests, such as bone scintigraphy, labeled leukocyte, and gallium scanning, suffer from relatively poor spatial resolution and lack sensitivity, specificity, or both. Initial data show that [(18)F]-FDG PET is an emerging imaging technique for diagnosing SI. [(18)F]-FDG PET appears to be especially helpful in those cases in which MRI cannot be performed or is non-diagnostic, and as an adjunct in patients in whom the diagnosis is inconclusive. The article reviews the currently available literature on [(18)F]-FDG PET and PET/CT in the diagnosis of SI.
Figures
References
-
- Adatepe MH, Powell OM, Isaacs GH, Nichols K, Cefola R. Hematogenous pyogenic vertebral osteomyelitis: diagnostic value of radionuclide bone imaging. J Nucl Med. 1986;27:1680–1685. - PubMed
-
- Aydinli U, Karaeminogullari O, Tiskaya K. Postoperative deep wound infection in instrumented spinal surgery. Acta Orthop Belg. 1999;65:182–187. - PubMed
-
- Boden SD, Davis DO, Dina TS, Sunner JL, Wiesel SW. Postoperative diskitis: distinguishing early MR imaging findings from normal postoperative disk space changes. Radiology. 1992;184:765–771. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
