

Ultra-early predictive assay for treatment failure using functional magnetic resonance imaging and clinical prognostic parameters in cervical cancer
- PMID: 20052727
- PMCID: PMC4362726
- DOI: 10.1002/cncr.24822
Ultra-early predictive assay for treatment failure using functional magnetic resonance imaging and clinical prognostic parameters in cervical cancer
Abstract
Background: The authors prospectively evaluated magnetic resonance imaging (MRI) parameters quantifying heterogeneous perfusion pattern and residual tumor volume early during treatment in cervical cancer, and compared their predictive power for primary tumor recurrence and cancer death with the standard clinical prognostic factors. A novel approach of augmenting the predictive power of clinical prognostic factors with MRI parameters was assessed.
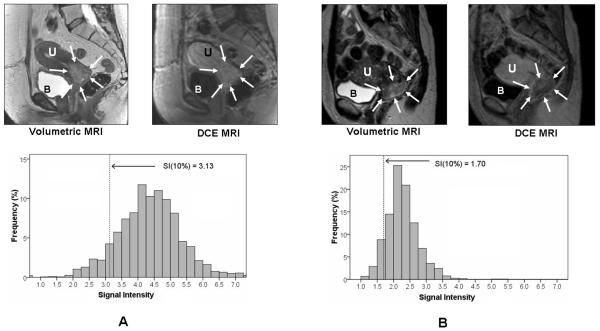
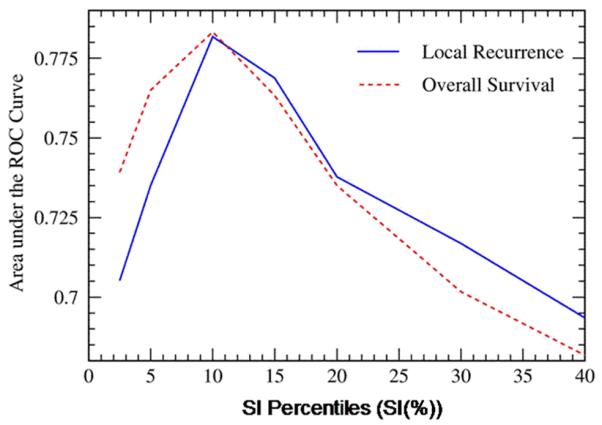
Methods: Sixty-two cervical cancer patients underwent dynamic contrast-enhanced (DCE) MRI before and during early radiation/chemotherapy (2-2.5 weeks into treatment). Heterogeneous tumor perfusion was analyzed by signal intensity (SI) of each tumor voxel. Poorly perfused tumor regions were quantified as lower 10th percentile of SI (SI[10%]). DCE-MRI and 3-dimensional (3D) tumor volumetry MRI parameters were assessed as predictors of recurrence and cancer death (median follow-up, 4.1 years). Their discriminating capacity was compared with clinical prognostic factors (stage, lymph node status, histology) using sensitivity/specificity and Cox regression analysis.
Results: SI(10%) and 3D volume 2-2.5 weeks into therapy independently predicted disease recurrence (hazard ratio [HR], 2.6; 95% confidence interval [95% CI], 1.0-6.5 [P = .04] and HR, 1.9; 95% CI, 1.1-3.5 [P = .03], respectively) and death (HR, 1.9; 95% CI, 1.0-3.5 [P = .03] and HR, 1.9; 95% CI, 1.2-2.9 [P = .01], respectively), and were superior to clinical prognostic factors. The addition of MRI parameters to clinical prognostic factors increased sensitivity and specificity of clinical prognostic factors from 71% and 51%, respectively, to 100% and 71%, respectively, for predicting recurrence, and from 79% and 54%, respectively, to 93% and 60%, respectively, for predicting death.
Conclusions: MRI parameters reflecting heterogeneous tumor perfusion and subtle tumor volume change early during radiation/chemotherapy are independent and better predictors of tumor recurrence and death than clinical prognostic factors. The combination of clinical prognostic factors and MRI parameters further improves early prediction of treatment failure and may enable a window of opportunity to alter treatment strategy.
Figures
Similar articles
-
Predicting control of primary tumor and survival by DCE MRI during early therapy in cervical cancer.Invest Radiol. 2009 Jun;44(6):343-50. doi: 10.1097/RLI.0b013e3181a64ce9. Invest Radiol. 2009. PMID: 19661844 Free PMC article.
-
Sequential magnetic resonance imaging of cervical cancer: the predictive value of absolute tumor volume and regression ratio measured before, during, and after radiation therapy.Cancer. 2010 Nov 1;116(21):5093-101. doi: 10.1002/cncr.25260. Cancer. 2010. PMID: 20629080 Free PMC article.
-
Longitudinal changes in tumor perfusion pattern during the radiation therapy course and its clinical impact in cervical cancer.Int J Radiat Oncol Biol Phys. 2010 Jun 1;77(2):502-8. doi: 10.1016/j.ijrobp.2009.04.084. Epub 2009 Sep 21. Int J Radiat Oncol Biol Phys. 2010. PMID: 19775824
-
Added-value of dynamic contrast-enhanced MRI on prediction of tumor recurrence in locally advanced cervical cancer treated with chemoradiotherapy.Eur Radiol. 2022 Apr;32(4):2529-2539. doi: 10.1007/s00330-021-08279-w. Epub 2021 Oct 13. Eur Radiol. 2022. PMID: 34647177
-
Extended-field radiotherapy for locally advanced cervical cancer.Cochrane Database Syst Rev. 2018 Oct 26;10(10):CD012301. doi: 10.1002/14651858.CD012301.pub2. Cochrane Database Syst Rev. 2018. PMID: 30362204 Free PMC article.
Cited by
-
Image-guided radiotherapy: from current concept to future perspectives.Nat Rev Clin Oncol. 2012 Dec;9(12):688-99. doi: 10.1038/nrclinonc.2012.194. Epub 2012 Nov 20. Nat Rev Clin Oncol. 2012. PMID: 23165124 Review.
-
Utilization of functional MRI in the diagnosis and management of cervical cancer.Front Oncol. 2022 Nov 11;12:1030967. doi: 10.3389/fonc.2022.1030967. eCollection 2022. Front Oncol. 2022. PMID: 36439416 Free PMC article. Review.
-
MR molecular imaging of tumor vasculature and vascular targets.Adv Genet. 2010;69:1-30. doi: 10.1016/S0065-2660(10)69010-4. Adv Genet. 2010. PMID: 20807600 Free PMC article. Review.
-
Imaging tumor hypoxia to advance radiation oncology.Antioxid Redox Signal. 2014 Jul 10;21(2):313-37. doi: 10.1089/ars.2013.5759. Epub 2014 Mar 24. Antioxid Redox Signal. 2014. PMID: 24329000 Free PMC article. Review.
-
Characterizing tumor heterogeneity with functional imaging and quantifying high-risk tumor volume for early prediction of treatment outcome: cervical cancer as a model.Int J Radiat Oncol Biol Phys. 2012 Jul 1;83(3):972-9. doi: 10.1016/j.ijrobp.2011.08.011. Epub 2011 Dec 28. Int J Radiat Oncol Biol Phys. 2012. PMID: 22208967 Free PMC article.
References
-
- Benedet JL, Bender H, Jones H, III, et al. FIGO staging classifications and clinical practice guidelines in the management of gynaecologic cancers. FIGO Committee Gynecologic Oncology. Int J Gynecol Obstet. 2000;70:209–262. - PubMed
-
- Delgado G, Bundy B, Zaino R, et al. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: a Gynecologic Oncology Group study. Gynecol Oncol. 1990;38:352–357. - PubMed
-
- Eifel PJ, Burke TW, Morris M, et al. Adenocarcinoma as an independent risk factor for disease recurrence in patients with stage IB cervical carcinoma. Gynecol Oncol. 1995;59:38–44. - PubMed
-
- Eifel PJ. Problems with the clinical staging of carcinoma of the cervix. Sem in Radiat Oncol. 1994;4:1–8. - PubMed
-
- vanNagell JR, Jr, Roddick JW, Jr, DM L. The staging of cervical cancer: inevitable discrepancies between clinical staging and pathologic findings. Am J Obstet Gynecol. 1971;110:973–978. - PubMed
