

Three-month follow-up of brief computerized and therapist interventions for alcohol and violence among teens
- PMID: 20053240
- PMCID: PMC2981597
- DOI: 10.1111/j.1553-2712.2009.00513.x
Three-month follow-up of brief computerized and therapist interventions for alcohol and violence among teens
Abstract
Objectives: Alcohol use and violent behaviors are well documented among adolescents and have enormous effects on morbidity and mortality. The authors hypothesized that universal computer screening of teens in an inner-city emergency department (ED), followed by a brief intervention (BI), would be 1) feasible (as measured by participation and completion of BI during the ED visit) and well received by teens (as measured by posttest process measures of intervention acceptability) and 2) effective at changing known precursors to behavior change such as attitudes, self-efficacy, and readiness to change alcohol use and violence.
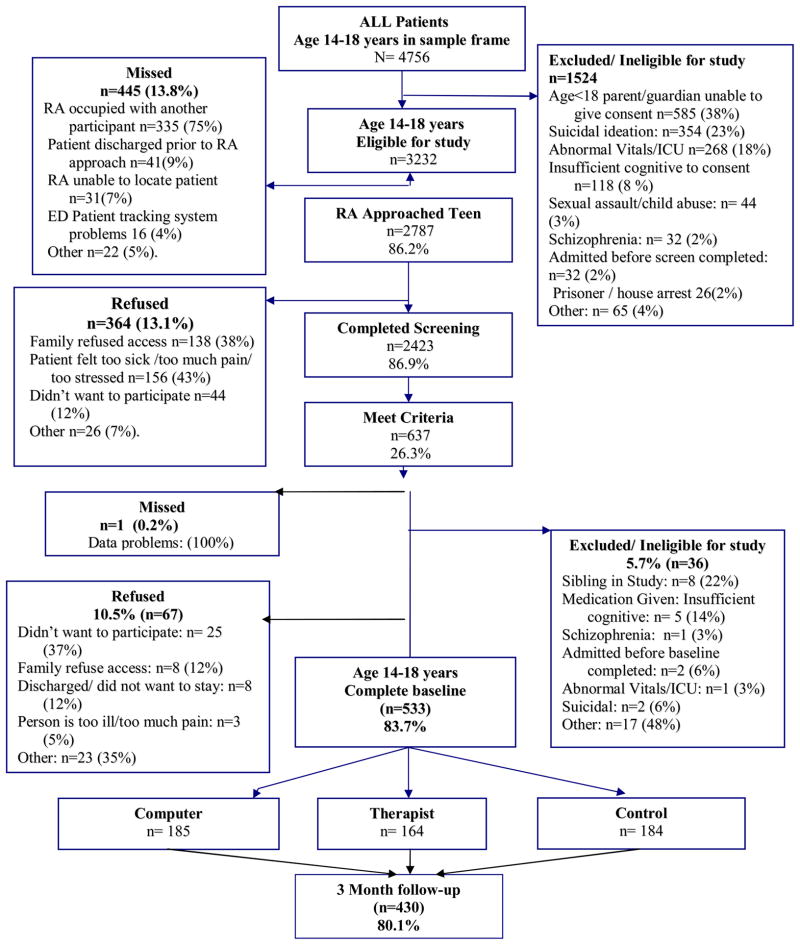
Methods: Adolescent patients (ages 14-18 years) at an urban ED were approached to complete a computerized survey. The survey was conducted daily from 12 noon to 11 pm from September 2006 through November 2008. Adolescents reporting both alcohol use and violence in the past year were randomized to a control group or a 35-minute BI delivered by a computer or therapist as part of the SafERteens study. Validated measures were administered, including demographics, alcohol use, attitudes toward alcohol and violence, self-efficacy for alcohol and violence, readiness to change alcohol and violence, and process questions, including likeability of intervention.
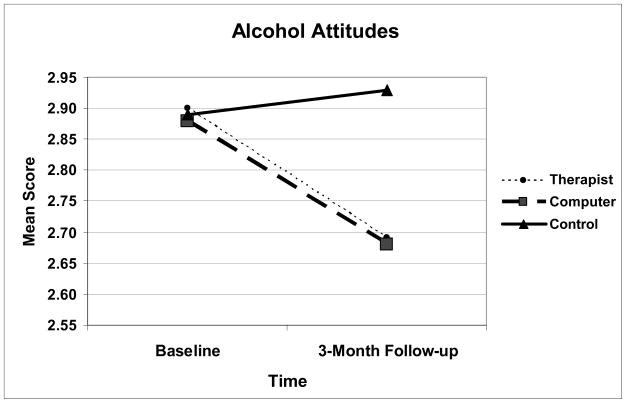
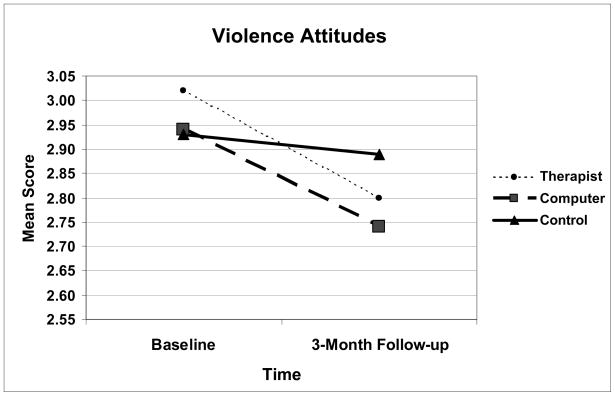
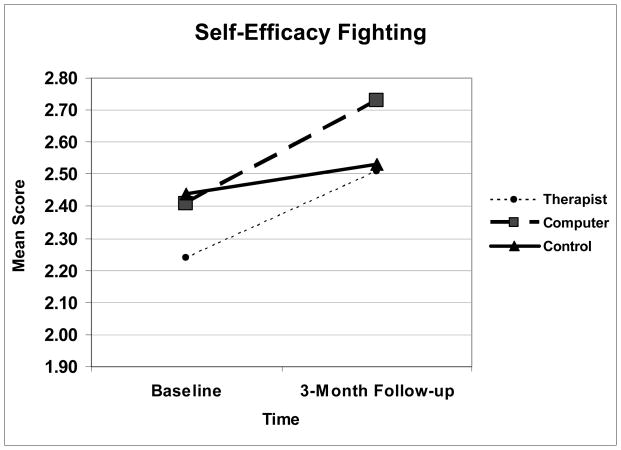
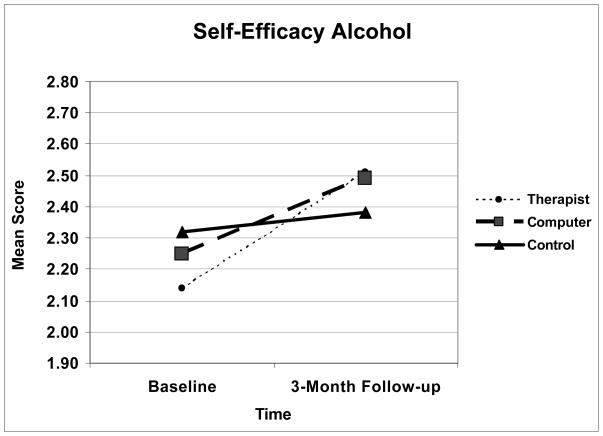
Results: A total of 2,423 adolescents were screened. Thirteen percent of those approached refused. The population was 45% male, 58% African American, and 6.2% Hispanic. Of those screened, 637 adolescents (26%) screened positive; 533 were randomized to participate, and 515 completed the BI prior to discharge. The BIs were well received by the adolescents overall; 97% of those randomized to a BI self-reported that they found one intervention section "very helpful." At posttest, significant reductions in positive attitudes for alcohol use and violence and significant increases in self-efficacy related to alcohol/violence were found for both therapist and computer interventions. At 3-month follow-up there was 81% retention, and generalized estimating equations (GEE) analysis showed that participants in both interventions had significant reductions in positive attitudes for alcohol use (therapist p = 0.002, computer p = 0.0001) and violence (therapist p = 0.012, computer p = 0.007) and significant increases in self-efficacy related to violence (therapist p = 0.0.04, computer p = 0.002); alcohol self-efficacy improved in the therapist BI condition only (therapist p = 0.050, computer p = 0.083). Readiness to change was not significantly improved.
Conclusions: This initial evaluation of the SafERteens study shows that universal computerized screening and BI for multiple risk behaviors among adolescents is feasible, well received, and effective at altering attitudes and self-efficacy. Future evaluations of the SafERteens study will evaluate the interventions' effects on behavioral change (alcohol use and violence) over the year following the ED visit.
(c) 2009 by the Society for Academic Emergency Medicine.
Figures
References
-
- National Center for Health Statistics & U.S. Health Care Financing Administration. The International Classification of Diseases, 9th Revision, Clinical Modification: ICD-9-CM. Washington, D.C.: US Department of Health and Human Services, Public Health Service; 2000.
-
- National Adolescent Health Information Center (NAHIC) fact sheet on mortality: Adolescents and young adults. 2006. [Accessed March 28, 2008]. Available at: http://nahic.ucsf.edu/download.php?f=/downloads/UnintInjury.pdf.
-
- Centers for Disease Control and Prevention. WISQARS Leading Causes of Death Reports, 1999–2002. [Accessed December 21, 2005]. 2005.
-
- Posner JC, Hawkins LA, Garcia-Espana F, et al. A randomized, clinical trial of a home safety intervention based in an emergency department setting. Pediatrics. 2004 Jun;113(6):1603–1608. - PubMed
-
- Johnston BD, Rivara FP, Droesch RM, et al. Behavior change counseling in the emergency department to reduce injury risk: a randomized, controlled trial. Pediatrics. 2002 Aug;110(2 Pt 1):267–274. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
