

Study protocol of the YOU CALL--WE CALL TRIAL: impact of a multimodal support intervention after a "mild" stroke
- PMID: 20053273
- PMCID: PMC2818655
- DOI: 10.1186/1471-2377-10-3
Study protocol of the YOU CALL--WE CALL TRIAL: impact of a multimodal support intervention after a "mild" stroke
Abstract
Background: More than 60% of new strokes each year are "mild" in severity and this proportion is expected to rise in the years to come. Within our current health care system those with "mild" stroke are typically discharged home within days, without further referral to health or rehabilitation services other than advice to see their family physician. Those with mild stroke often have limited access to support from health professionals with stroke-specific knowledge who would typically provide critical information on topics such as secondary stroke prevention, community reintegration, medication counselling and problem solving with regard to specific concerns that arise. Isolation and lack of knowledge may lead to a worsening of health problems including stroke recurrence and unnecessary and costly health care utilization.The purpose of this study is to assess the effectiveness, for individuals who experience a first "mild" stroke, of a sustainable, low cost, multimodal support intervention (comprising information, education and telephone support)--"WE CALL" compared to a passive intervention (providing the name and phone number of a resource person available if they feel the need to)--"YOU CALL", on two primary outcomes: unplanned-use of health services for negative events and quality of life.
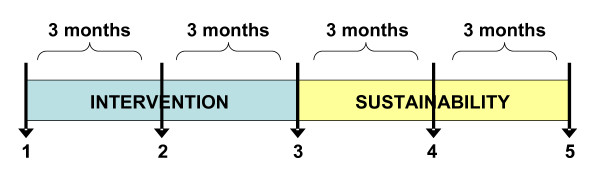
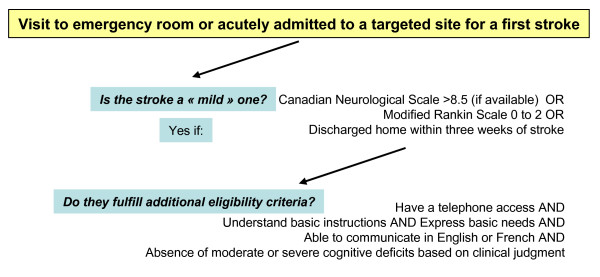
Method/design: We will recruit 384 adults who meet inclusion criteria for a first mild stroke across six Canadian sites. Baseline measures will be taken within the first month after stroke onset. Participants will be stratified according to comorbidity level and randomised to one of two groups: YOU CALL or WE CALL. Both interventions will be offered over a six months period. Primary outcomes include unplanned use of heath services for negative event (frequency calendar) and quality of life (EQ-5D and Quality of Life Index). Secondary outcomes include participation level (LIFE-H), depression (Beck Depression Inventory II) and use of health services for health promotion or prevention (frequency calendar). Blind assessors will gather data at mid-intervention, end of intervention and one year follow up.
Discussion: If effective, this multimodal intervention could be delivered in both urban and rural environments. For example, existing infrastructure such as regional stroke centers and existing secondary stroke prevention clinics, make this intervention, if effective, deliverable and sustainable.
Trial registration: ISRCTN95662526.
Figures
References
-
- Jones MR, Horner RD, Edwards LJ, Hoff J, Armstrong SB, Smith-Hammond CA. Racial variation in initial stroke severity. Stroke; a journal of cerebral circulation. 2000;31(3):563–7. - PubMed
-
- Sturm JW, Donnan GA, Dewey HM, Macdonell RA, Gilligan AK, Thrift AG. Determinants of handicap after stroke: the North East Melbourne Stroke Incidence Study (NEMESIS) Stroke; a journal of cerebral circulation. 2004;35(3):715–20. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
