

Plasmodium falciparum resistance to anti-malarial drugs in Papua New Guinea: evaluation of a community-based approach for the molecular monitoring of resistance
- PMID: 20053293
- PMCID: PMC2820042
- DOI: 10.1186/1475-2875-9-8
Plasmodium falciparum resistance to anti-malarial drugs in Papua New Guinea: evaluation of a community-based approach for the molecular monitoring of resistance
Abstract
Background: Molecular monitoring of parasite resistance has become an important complementary tool in establishing rational anti-malarial drug policies. Community surveys provide a representative sample of the parasite population and can be carried out more rapidly than accrual of samples from clinical cases, but it is not known whether the frequencies of genetic resistance markers in clinical cases differ from those in the overall population, or whether such community surveys can provide good predictions of treatment failure rates.
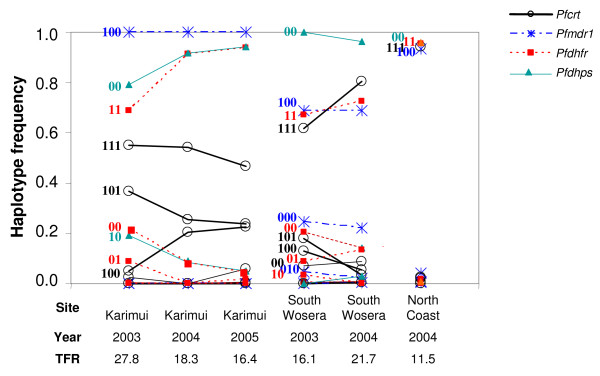
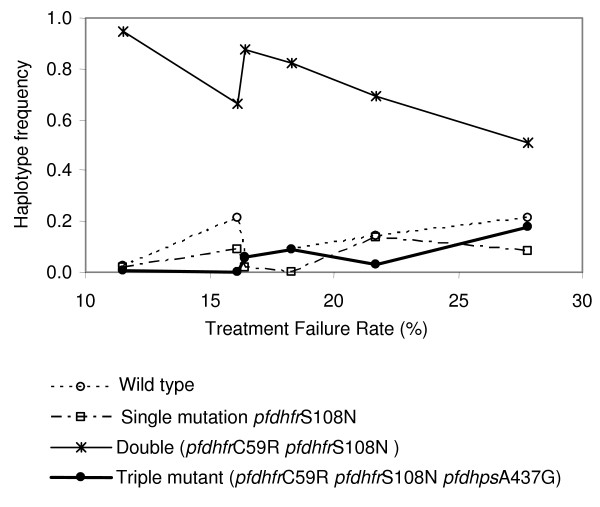
Methods: Between 2003 and 2005, in vivo drug efficacy of amodiaquine or chloroquine plus sulphadoxine-pyrimethamine was determined at three sites in Papua New Guinea. The genetic drug resistance profile (i.e., 33 single nucleotide polymorphisms in Plasmodium falciparum crt, mdr1, dhfr, dhps, and ATPase6) was concurrently assessed in 639 community samples collected in the catchment areas of the respective health facilities by using a DNA microarray-based method. Mutant allele and haplotype frequencies were determined and their relationship with treatment failure rates at each site in each year was investigated.
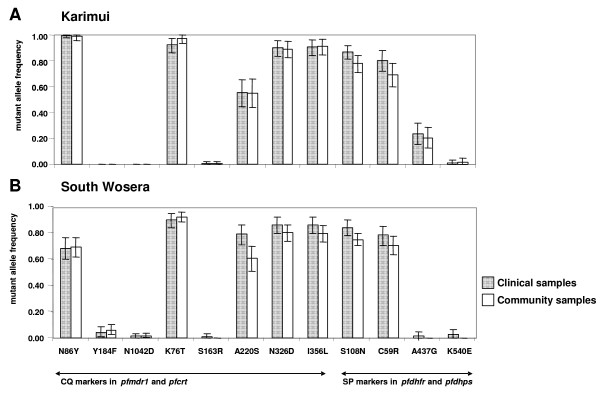
Results: PCR-corrected in vivo treatment failure rates were between 12% and 28% and varied by site and year with variable longitudinal trends. In the community samples, the frequencies of mutations in pfcrt and pfmdr1 were high and did not show significant changes over time. Mutant allele frequencies in pfdhfr were moderate and those in pfdhps were low. No mutations were detected in pfATPase6. There was much more variation between sites than temporal, within-site, variation in allele and haplotype frequencies. This variation did not correlate well with treatment failure rates. Allele and haplotype frequencies were very similar in clinical and community samples from the same site.
Conclusions: The relationship between parasite genetics and in vivo treatment failure rate is not straightforward. The frequencies of genetic anti-malarial resistance markers appear to be very similar in community and clinical samples, but cannot be used to make precise predictions of clinical outcome. Thus, indicators based on molecular data have to be considered with caution and interpreted in the local context, especially with regard to prior drug usage and level of pre-existing immunity. Testing community samples for molecular drug resistance markers is a complementary tool that should help decision-making for the best treatment options and appropriate potential alternatives.
Figures
References
-
- Hastings IM. Molecular markers as indicators of antimalarial drug failure rates. Trop Med Int Health. 2007;12:1298–1301. - PubMed
-
- Plowe CV, Roper C, Barnwell JW, Happi CT, Joshi HH, Mbacham W, Meshnick SR, Mugittu K, Naidoo I, Price RN, Shafer RW, Sibley CH, Sutherland CJ, Zimmerman PA, Rosenthal PJ. World Antimalarial Resistance Network (WARN) III: molecular markers for drug resistant malaria. Malar J. 2007;6:121. doi: 10.1186/1475-2875-6-121. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
