

The 5-year direct medical cost of neonatal and childhood stroke in a population-based cohort
- PMID: 20054007
- PMCID: PMC2816005
- DOI: 10.1212/WNL.0b013e3181cbcd48
The 5-year direct medical cost of neonatal and childhood stroke in a population-based cohort
Abstract
Background: Despite increasing awareness of the long-term impact of pediatric stroke, there are few estimates of the costs of care. We examined acute and 5-year direct costs of neonatal and childhood stroke in a population-based cohort in Northern California.
Methods: We obtained electronic cost data for 266 children with neurologist-confirmed strokes, and 786 age-matched stroke-free controls, within the population of all children (<20 years) enrolled in a large managed care plan from 1996 through 2003. Cost data included all inpatient and outpatient health service costs including care at out-of-plan facilities. Costs were assessed for 5 years after stroke, expressed in 2003 US dollars, and stratified by age at stroke onset (neonatal, defined as <29 days of life, vs childhood). Stroke costs were adjusted for costs in stroke-free age-matched controls.
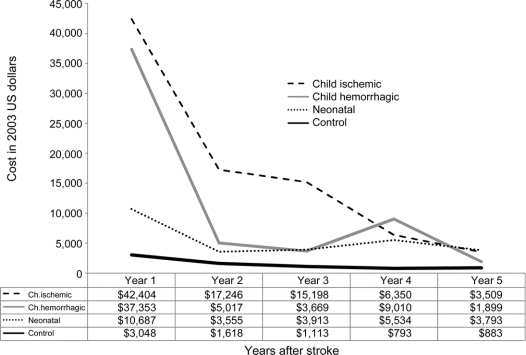
Results: Average adjusted 5-year costs for pediatric stroke are substantial: $51,719 for neonatal stroke and $135,161 for childhood stroke. The average cost of a childhood stroke admission was $81,869. The average birth admission cost for a neonatal stroke was $39,613; adjustment for control birth admission costs reduced this by only $4,792, suggesting the stroke accounted for 88% of costs. Even among neonates whose strokes were not recognized until later in childhood ("presumed perinatal strokes"), admission costs exceeded those of controls. Chronic costs were highest in the first year poststroke, but continued to exceed control costs even in the fifth year by an average of $2,016.
Conclusions: The economic burden of neonatal and childhood stroke is both large and sustained.
Figures
References
-
- deVeber GA, MacGregor D, Curtis R, Mayank S. Neurologic outcome in survivors of childhood arterial ischemic stroke and sinovenous thrombosis. J Child Neurol 2000;15:316–324. - PubMed
-
- Hartel C, Schilling S, Sperner J, Thyen U. The clinical outcomes of neonatal and childhood stroke: review of the literature and implications for future research. Eur J Neurol 2004;11:431–438. - PubMed
-
- Lee J, Croen LA, Backstrand KH, et al. Maternal and infant characteristics associated with perinatal arterial stroke in the infant. JAMA 2005;293:723–729. - PubMed
-
- Fullerton HJ, Wu YW, Zhao S, Johnston SC. Risk of stroke in children: ethnic and gender disparities. Neurology 2003;61:189–194. - PubMed
-
- Fullerton HJ, Chetkovich DM, Wu YW, Smith WS, Johnston SC. Deaths from stroke in US children, 1979 to 1998. Neurology 2002;59:34–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical