

Changing from bevacizumab to ranibizumab in age-related macular degeneration. Is it safe?
- PMID: 20054410
- PMCID: PMC2801585
- DOI: 10.2147/cia.s8367
Changing from bevacizumab to ranibizumab in age-related macular degeneration. Is it safe?
Abstract
Objective: To report our experiences in changing from intravitreal bevacizumab to ranibizumab in age-related macular degeneration (AMD).
Design: Retrospective case series.
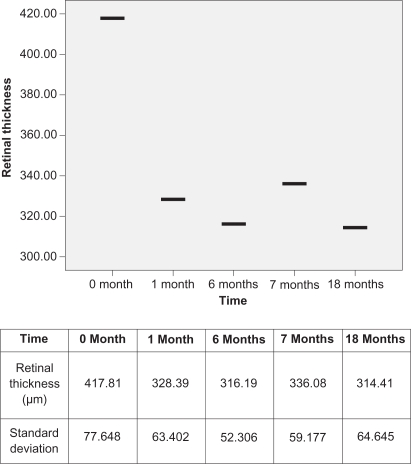
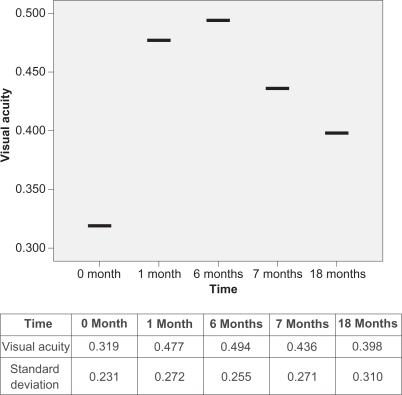
Participants and methods: We retrospectively reviewed the records of 34 patients (36 eyes) who were treated with monthly injections of intravitreal bevacizumab for six months and then switched to monthly injections of ranibizumab for 12 months. Best-corrected visual acuity measurements (BCVA), contact lens biomicroscopy, optical coherence tomography (OCT), and fluorescein angiography were performed at the baseline examination and then monthly. Chi-square test was used for statistical analysis.
Results: Following bevacizumab treatment, retinal thickness decreased (P = 0.033) while BCVA improved (P = 0.040). Changing from bevacizumab to ranibizumab resulted in a transient decrease in BCVA (P = 0.045) and an increase in retinal thickness (P = 0.042). In addition, three eyes presented with a large subretinal hemorrhage. However, final retinal thickness was better than the initial thickness and the value following the bevacizumab course. No major ocular or systemic side effects were noted.
Conclusions: Ranibizumab was clinically effective in the long term but the change of treatment from bevacizumab to a half-size molecule with less half-life in the vitreous such as ranibizumab contributed to a transient "instability" in the eye which may have triggered the large subretinal hemorrhage. There is insufficient experience reported in the literature in switching from one agent to another. A prospective study with controls is necessary to determine whether it is safe to change from one medication to another.
Keywords: age-related macular degeneration; bevacizumab; ranibizumab; subretinal hemorrhage.
Figures
Similar articles
-
Large subretinal haemorrhage following change from intravitreal bevacizumab to ranibizumab.Ophthalmologica. 2009;223(4):279-82. doi: 10.1159/000213644. Epub 2009 Apr 22. Ophthalmologica. 2009. PMID: 19390227
-
Comparative study of intravitreal bevacizumab (Avastin) versus ranibizumab (Lucentis) in the treatment of neovascular age-related macular degeneration.Ophthalmologica. 2009;223(6):370-5. doi: 10.1159/000227783. Epub 2009 Jul 8. Ophthalmologica. 2009. PMID: 19590252
-
Treatment of neovascular age-related macular degeneration with a variable ranibizumab dosing regimen and one-time reduced-fluence photodynamic therapy: the TORPEDO trial at 2 years.Graefes Arch Clin Exp Ophthalmol. 2010 Jul;248(7):943-56. doi: 10.1007/s00417-009-1256-6. Epub 2010 Mar 4. Graefes Arch Clin Exp Ophthalmol. 2010. PMID: 20204659 Clinical Trial.
-
Off-label use of bevacizumab for the treatment of age-related macular degeneration: what is the evidence?Drugs Aging. 2009;26(4):295-320. doi: 10.2165/00002512-200926040-00002. Drugs Aging. 2009. PMID: 19476398 Review.
-
Uveitis, the Comparison of Age-Related Macular Degeneration Treatments Trials (CATT), and intravitreal biologics for ocular inflammation.Am J Ophthalmol. 2012 Sep;154(3):429-435.e2. doi: 10.1016/j.ajo.2012.05.011. Am J Ophthalmol. 2012. PMID: 22898344 Free PMC article. Review.
Cited by
-
Lasting controversy on ranibizumab and bevacizumab.Theranostics. 2011;1:395-402. doi: 10.7150/thno/v01p0395. Epub 2011 Dec 12. Theranostics. 2011. PMID: 22211145 Free PMC article.
-
Clinical Outcomes of Retinal Arterial Macroaneurysms With Vitreous Hemorrhage Treated With Observation, Antivascular Endothelial Growth Factor Intravitreal Injections, or Pars Plana Vitrectomy.J Vitreoretin Dis. 2023 Oct 3;7(6):483-489. doi: 10.1177/24741264231200734. eCollection 2023 Nov-Dec. J Vitreoretin Dis. 2023. PMID: 37974920 Free PMC article.
-
Switching from intravitreal ranibizumab to bevacizumab for age-related macular degeneration.ISRN Ophthalmol. 2011 Dec 21;2011:916789. doi: 10.5402/2011/916789. eCollection 2011. ISRN Ophthalmol. 2011. PMID: 24555120 Free PMC article.
-
The proliferation of malignant melanoma cells could be inhibited by ranibizumab via antagonizing VEGF through VEGFR1.Mol Vis. 2014 May 13;20:649-60. eCollection 2014. Mol Vis. 2014. PMID: 24868139 Free PMC article.
-
Subretinal recombinant tissue plasminogen activator and pneumatic displacement for the management of subretinal hemorrhage occurring after anti-VEGF injections for wet AMD.Clin Ophthalmol. 2011;5:459-63. doi: 10.2147/OPTH.S15864. Epub 2011 Apr 13. Clin Ophthalmol. 2011. PMID: 21573092 Free PMC article.
References
-
- Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP. Age-related macular degeneration: etiology, pathogenesis, and therapeutic strategies. Surv Ophthalmol. 2003;48(3):257–293. - PubMed
-
- Bressler NM, Bressler SB, Fine SL. Age-related macular degeneration. Surv Ophthalmol. 1988;32(6):375–413. - PubMed
-
- Guyer DR, Fine SL, Maguire MG, Hawkins BS, Owens SL, Murphy RP. Subfoveal choroidal neovascular membranes in age-related macular degeneration. Visual prognosis in eyes with relatively good initial visual acuity. Arch Ophthalmol. 1986;104(5):702–705. - PubMed
-
- Gatto B, Cavalli M. From proteins to nucleic acid-based drugs: the role of biotech in anti-VEGF therapy. Anticancer Agents Med Chem. 2006;6(4):287–301. - PubMed
-
- Gaudreault J, Fei D, Rusit J, Suboc P, Shiu V. Preclinical pharmacokinetics of Ranibizumab (rhuFabV2) after a single intravitreal administration. Invest Ophthalmol Vis Sci. 2005;46(2):726–733. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
