

BK-virus and the impact of pre-emptive immunosuppression reduction: 5-year results
- PMID: 20055811
- PMCID: PMC3188431
- DOI: 10.1111/j.1600-6143.2009.02952.x
BK-virus and the impact of pre-emptive immunosuppression reduction: 5-year results
Abstract
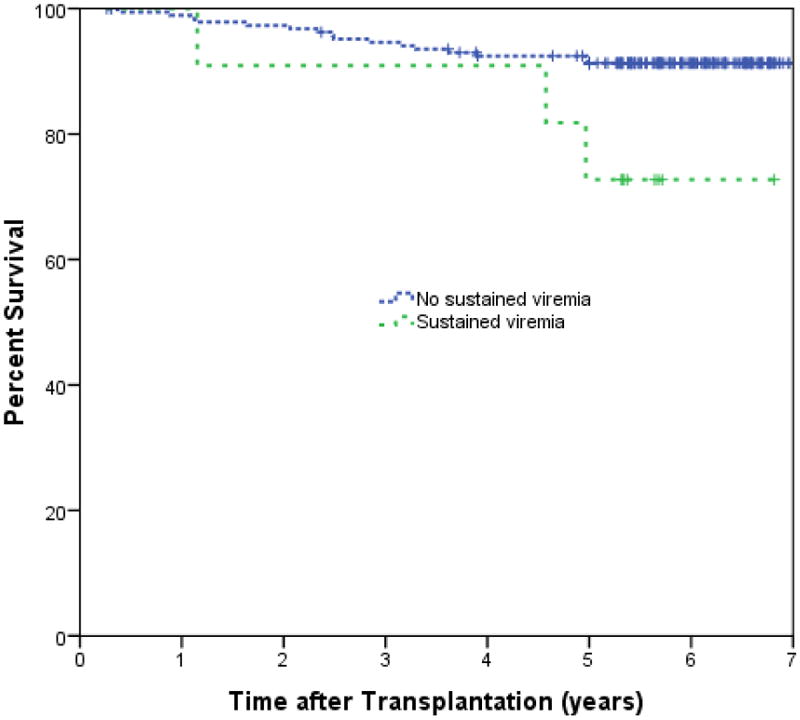
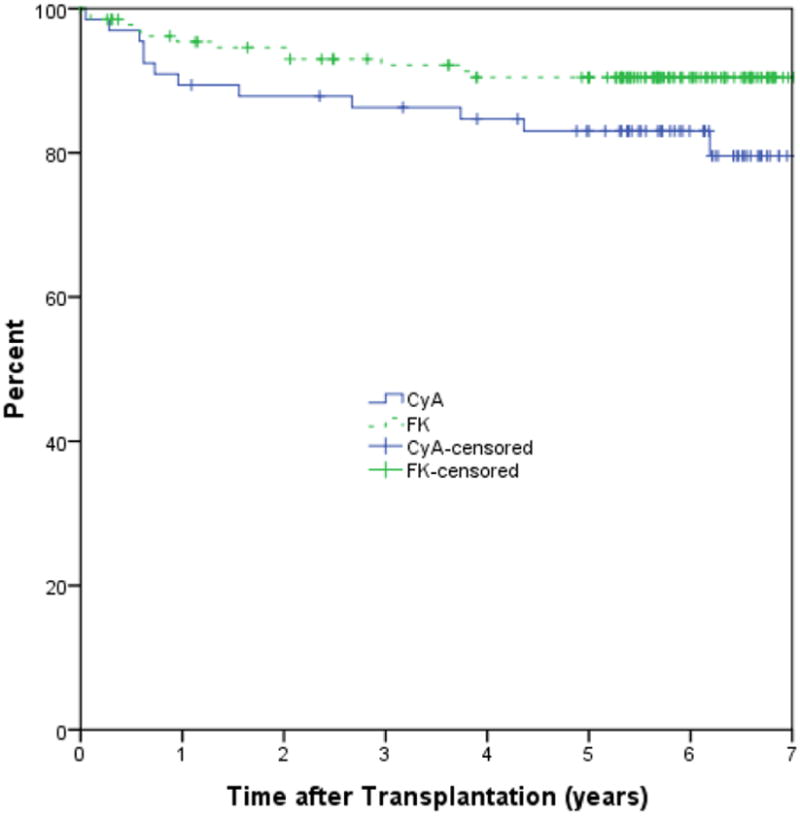
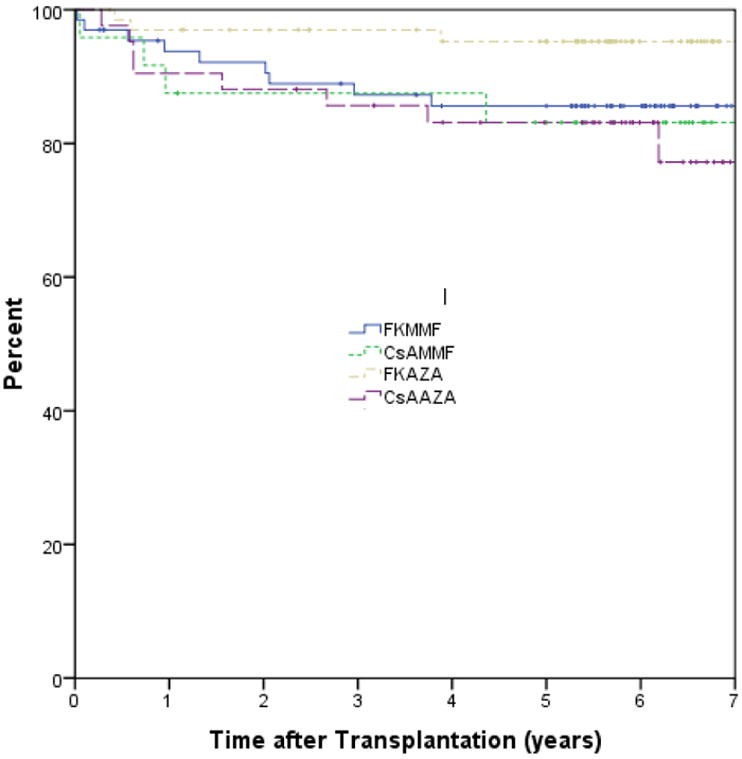
A 1-year, single-center, randomized trial demonstrated that the calcineurin inhibitor or adjuvant immunosuppression, independently, does not affect BK-viruria or viremia and that monitoring and pre-emptive withdrawal of immunosuppression was associated with resolution of BK-viremia and absence of clinical BK-nephropathy without acute rejection or graft loss. A retrospective 5-year review of this trial was conducted. In cases of BK viremia, the antimetabolite was withdrawn and for sustained viremia, the calcineurin inhibitor was minimized. Five-year follow-up was available on 97% of patients. Overall 5-year patient survival was 91% and graft survival was 84%. There were no differences in patient-survival by immunosuppressive regimen or presence of BK-viremia. Immunosuppression and viremia did not influence graft survival. Acute rejection occurred in 12% by 5-years after transplant, was less common with tacrolimus versus cyclosporine (9% vs. 18%; p = 0.082), and was lowest with the tacrolimus-azathioprine regimen (5%, p = 0.127). Tacrolimus was associated with better renal function at 5-years (eGFR 63 FK vs. 52 CsA mL/min, p = 0.001). Minimization of immunosuppression upon detection of BK-viremia was associated with excellent graft survival at 5-years, low rejection rates and excellent renal function. It is a safe, short and long-term strategy that resulted in freedom from clinically evident BK-virus nephropathy.
Figures
References
-
- Ramos E, Drachenberg CB, Portocarrero M, Wali R, Klassen DK, Fink JC, et al. BK virus nephropathy diagnosis and treatment: experience at the University of Maryland Renal Transplant Program. Clin Transpl. 2002:143–53. - PubMed
-
- Ramos E, Drachenberg CB, Papadimitriou JC, Hamze O, Fink JC, Klassen DK, et al. Clinical course of polyoma virus nephropathy in 67 renal transplant patients. J Am Soc Nephrol. 2002;13:2145–51. - PubMed
-
- Buehrig CK, Lager DJ, Stegall MD, Kreps MA, Kremers WK, Gloor JM, et al. Influence of surveillance renal allograft biopsy on diagnosis and prognosis of polyomavirus-associated nephropathy. Kidney Int. 2003;64:665–73. - PubMed
-
- Mengel M, Marwedel M, Radermacher J, Eden G, Schwarz A, Haller H, et al. Incidence of polyomavirus-nephropathy in renal allografts: influence of modern immunosuppressive drugs. Nephrol Dial Transplant. 2003;18:1190–96. - PubMed
-
- Gardner SD, Field AM, Coleman DV, Hulme B. New human papovavirus (B.K.) isolated from urine after renal transplantation. Lancet. 1971;1:1253–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
