

Association of paternal age and risk for major congenital anomalies from the National Birth Defects Prevention Study, 1997 to 2004
- PMID: 20056435
- PMCID: PMC2824069
- DOI: 10.1016/j.annepidem.2009.10.009
Association of paternal age and risk for major congenital anomalies from the National Birth Defects Prevention Study, 1997 to 2004
Abstract
Purpose: The objective of this study was to examine the associations between paternal age and birth defects of unknown etiologies while carefully controlling for maternal age.
Methods: By using 1997 to 2004 data from the National Birth Defects Prevention Study, we fit logistic regression models with paternal and maternal age as continuous variables while adjusting for demographic and other factors.
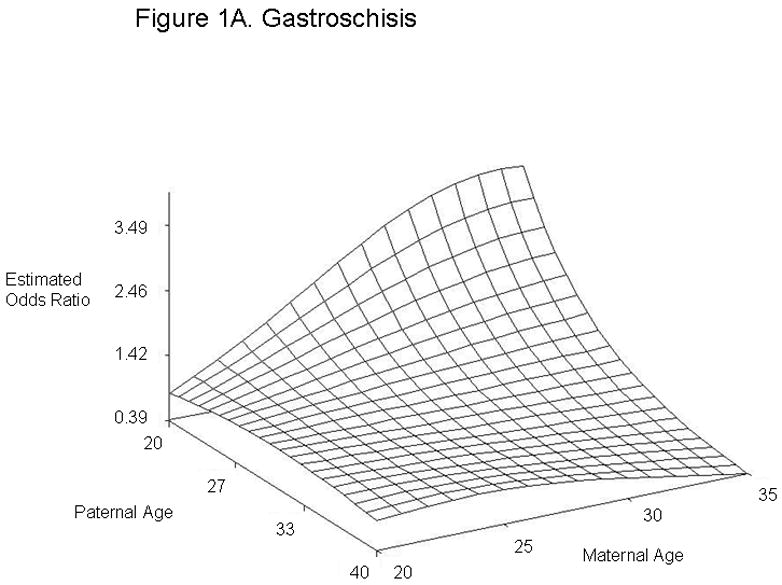
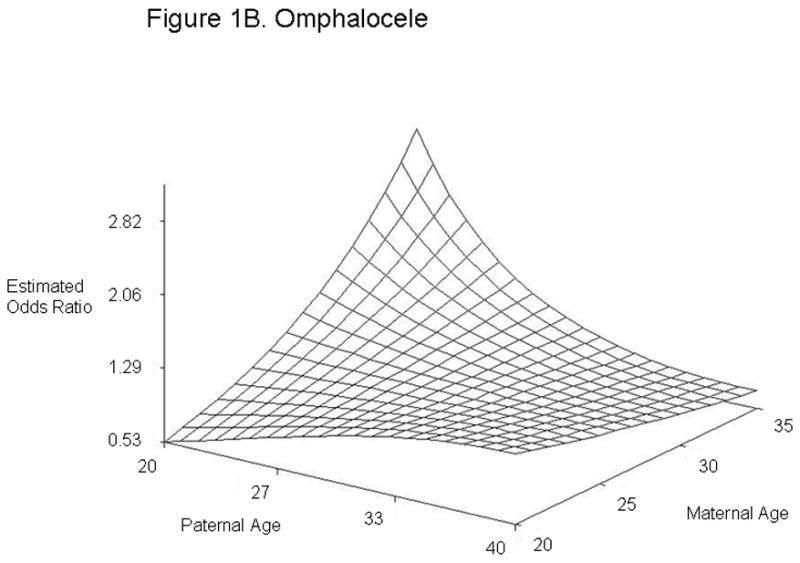
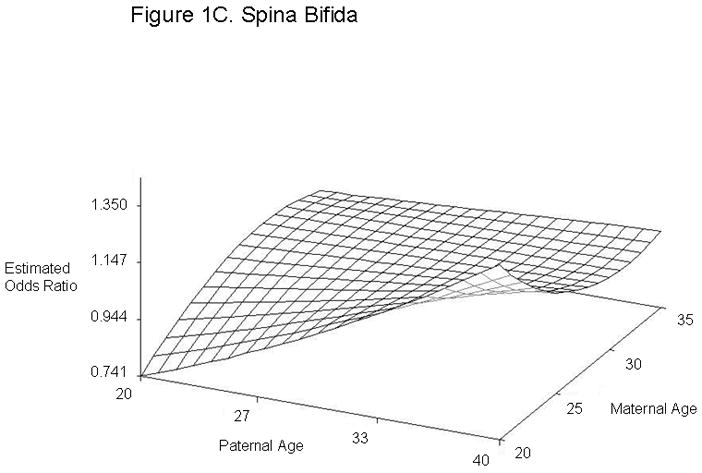
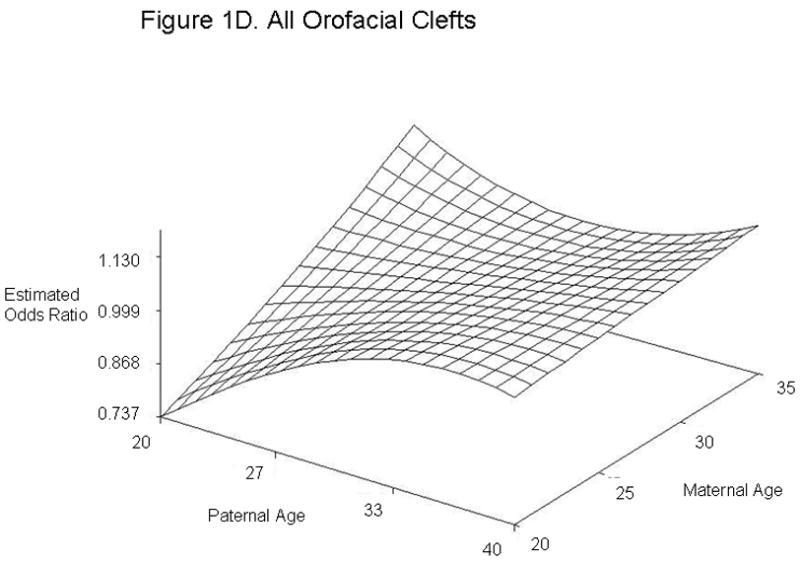
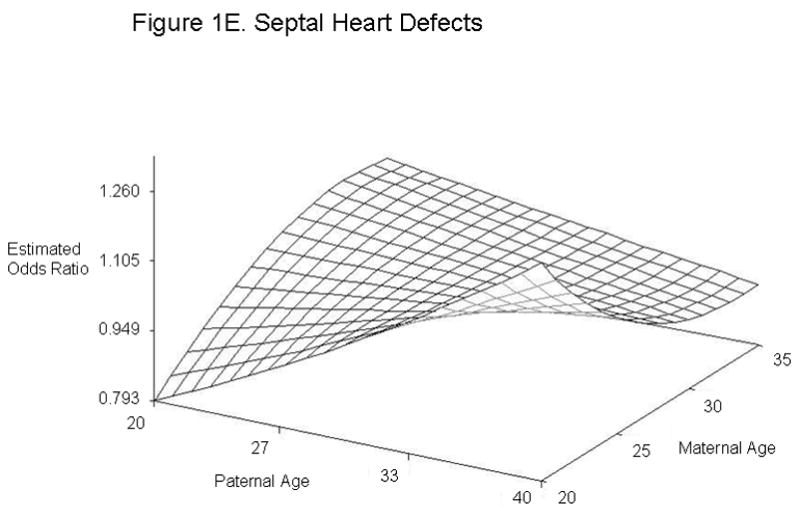
Results: Elevated odds ratios (ORs) for each year increase in paternal age were found for cleft palate (OR. 1.02, 95% confidence interval [95% CI], 1.00-1.04), diaphragmatic hernia (OR, 1.04; 95% CI, 1.02-1.06), right ventricular outflow tract obstruction (OR, 1.03; 95% CI, 1.01-1.04), and pulmonary valve stenosis (OR, 1.02, 95% CI, 1.01-1.04). At younger paternal ages, each year increase in paternal age correlated with increased odds of having offspring with encephalocele, cataract, esophageal atresia, anomalous pulmonary venous return, and coarctation of the aorta, but these increased odds were not observed at older paternal ages. The effect of paternal age was modified by maternal age for gastroschisis, omphalocele, spina bifida, all orofacial clefts, and septal heart defects.
Conclusions: Our findings suggest that paternal age may be a risk factor for some multifactorial birth defects.
Published by Elsevier Inc.
Figures
References
-
- Puscheck EE, Jeyendran RS. The impact of male factor on recurrent pregnancy loss. Curr Opin Obstet Gynecol. 2007;19:222–228. - PubMed
-
- Sartorelli EM, Mazzucatto LF, de Pina-Neto JM. Effect of paternal age on human sperm chromosomes. Fertil Steril. 2001;76:1119–1123. - PubMed
-
- Schmid TE, Eskenazi B, Baumgartner A, et al. The effects of male age on sperm DNA damage in healthy non-smokers. Hum Reprod. 2007;22:180–187. - PubMed
-
- de la Rochebrochard E, Thonneau P. Paternal age and maternal age are risk factors for miscarriage; results of a multicentre European study. Hum Reprod. 2002;17:1649–1656. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
