

Effect of different dialysis modalities on microinflammatory status and endothelial damage
- PMID: 20056757
- PMCID: PMC2827586
- DOI: 10.2215/CJN.03260509
Effect of different dialysis modalities on microinflammatory status and endothelial damage
Abstract
Background and objectives: We studied the relationship between microinflammation and endothelial damage in chronic kidney disease (CKD) patients on different dialysis modalities.
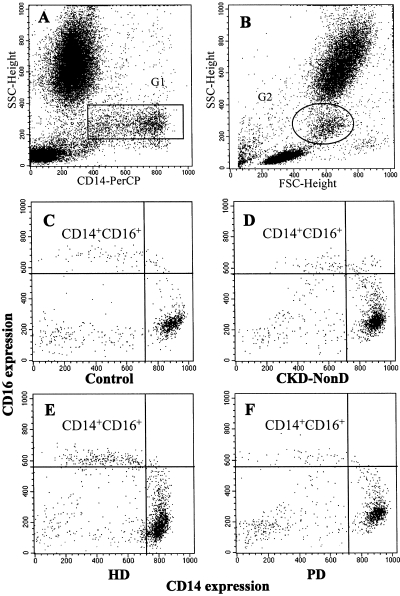
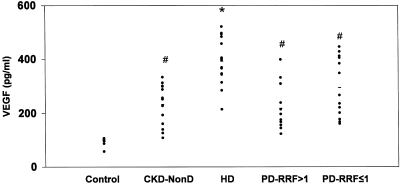
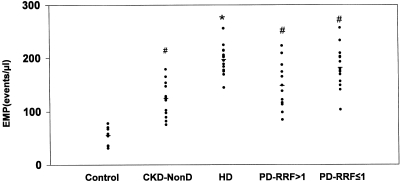
Design, setting, participants, & measurements: Four groups of CKD stage 5 patients were studied: 1) 14 nondialysis CKD patients (CKD-NonD); 2) 15 hemodialysis patients (HD); 3) 12 peritoneal dialysis patients with residual renal function >1 ml/min (PD-RRF >1); and 4) 13 peritoneal dialysis patients with residual renal function <or=1 ml/min (PD-RRF <or=1). Ten healthy subjects served as controls. CD14(+)CD16(+) cells and apoptotic endothelial microparticles (EMPs) were measured by flow cytometry. Serum vascular endothelial growth factor (VEGF) was measured by ELISA.
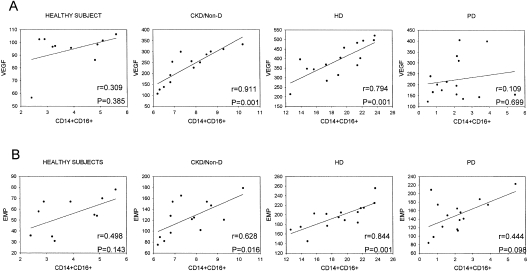
Results: CKD-NonD and HD patients had a higher percentage of CD14(+)CD16(+) monocytes than PD groups and controls. CD14(+)CD16(+) was similar in the PD groups, regardless of their RRF, and controls. The four uremic groups displayed a marked increase in apoptotic EMPs and VEGF compared with controls. Apoptotic EMPs and VEGF were significantly higher in HD patients than in CKD-NonD and both PD groups. However, there were no significant differences between CKD-NonD and the two PD groups. There was a correlation between CD14(+)CD16(+) and endothelial damage in CKD-NonD and HD patients, but not in PD and controls.
Conclusions: There was an increase in CD14(+)CD16(+) only in CKD-NonD and HD patients. In these patients, there was a relationship between increased CD14(+)CD16(+) and endothelial damage. These results strongly suggest that other factors unrelated to the microinflammatory status mediated by CD14(+)CD16(+) are promoting the endothelial damage in PD, regardless of their RRF.
Figures
References
-
- Foley RN, Parfrey PS, Sarnak MJ: Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol 9: S16–23, 1998 - PubMed
-
- Ma KW, Greene EL, Raij L: Cardiovascular risk factors in chronic renal failure and hemodialysis populations. Am J Kidney Dis 19: 505–513, 1992 - PubMed
-
- Lameire N, Bernaert P, Lambert MC, Vijt D: Cardiovascular risk factors and their management in patients on continuous ambulatory peritoneal dialysis. Kidney Int Suppl 48: S31–S38, 1994 - PubMed
-
- Den Elzen WP, van Manen JG, Boeschoten EW, Krediet RT, Dekker FW: The effect of single and repeatedly high concentrations of C-reactive protein on cardiovascular and non-cardiovascular mortality in patients starting with dialysis. Nephrol Dial Transplant 21: 1588–1595, 2006 - PubMed
-
- Papagianni A, Kokolina E, Kalovoulos M, Vainas A, Dimitriadis C, Memmos D: Carotid atherosclerosis is associated with inflammation, malnutrition and intercellular adhesion molecule-1 in patients on continuous ambulatory peritoneal dialysis. Nephrol Dial Transplant 19: 1258–1263, 2004 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
