

Improving the quality of colorectal cancer screening: assessment of familial risk
- PMID: 20058076
- PMCID: PMC2871248
- DOI: 10.1007/s10620-009-1058-z
Improving the quality of colorectal cancer screening: assessment of familial risk
Abstract
Background: Accuracy of familial risk assessment by endoscopists in determining colonoscopic screening and surveillance intervals is unknown.
Aims: To investigate follow-up recommended by endoscopists for individuals at average or increased familial risk, following colonoscopies that were normal or yielded hyperplastic polyps only.
Methods: Colonoscopy registry data was analyzed on 5,982 patients who had colonoscopy between 2004 and 2006. Patient information was linked with colonoscopy procedure information and pathology results. Patients with a personal or family history of colorectal cancer (CRC) or polyps, inflammatory bowel disease, or who had diagnostic, incomplete or suboptimally prepped examinations were excluded. The final analysis, which included 2,414 patients, investigated concordance of risk assessment between patient and endoscopist, and resulting endoscopist follow-up recommendations.
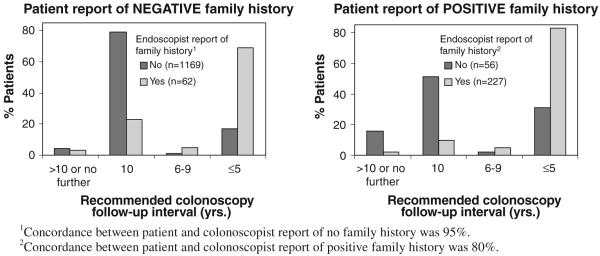
Results: Following normal colonoscopy, 76% of average risk individuals were told to follow-up in 10 years, but if a hyperplastic polyp was found, less than 10 years was suggested for 76%. Many patients reporting a known familial cancer syndrome or a very strong family history did not have that history indicated on the endoscopist's procedure form, and recommended follow-up intervals were beyond guideline recommendations for 60.4% of the very high-risk group.
Conclusions: Endoscopists may sometimes be unaware of the presence of familial risk factors, even for individuals at very high familial risk. Greater consistency and accuracy in familial risk assessments could significantly increase the efficacy of screening in preventing colorectal cancer.
Figures
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. CA Cancer J Clin. 2007;57(1):43–66. - PubMed
-
- Winawer SJ, Zauber AG, Ho MN, et al. The National Polyp Study Workgroup Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 1993;329(27):1977–1981. - PubMed
-
- Lang CA, Ransohoff DF. Fecal occult blood screening for colorectal cancer. Is mortality reduced by chance selection for screening colonoscopy? Jama. 1994;271(13):1011–1013. - PubMed
-
- Byers T, Levin B, Rothenberger D, Dodd GD, Smith RA, American Cancer Society Detection and Treatment Advisory Group on Colorectal Cancer American Cancer Society guidelines for screening and surveillance for early detection of colorectal polyps and cancer: update 1997. CA Cancer J Clin. 1997;47(3):154–160. - PubMed
-
- Seeff LC, Richards TB, Shapiro JA, et al. How many endoscopies are performed for colorectal cancer screening? Results from CDC’s survey of endoscopic capacity. Gastroenterology. 2004;127(6):1670–1677. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
