

Modeling progression in radiation-induced lung adenocarcinomas
- PMID: 20058155
- PMCID: PMC2855436
- DOI: 10.1007/s00411-009-0264-6
Modeling progression in radiation-induced lung adenocarcinomas
Abstract
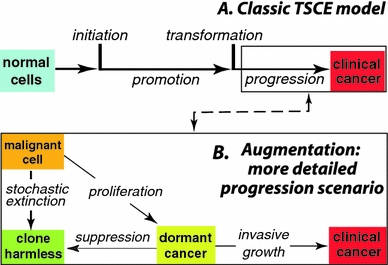
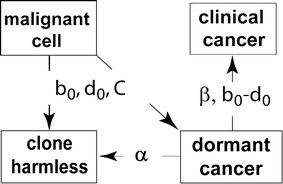
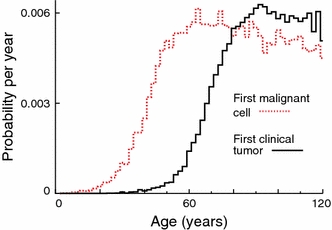
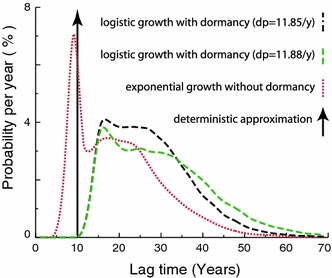
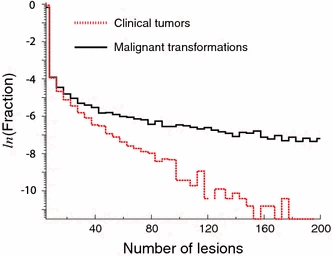
Quantitative multistage carcinogenesis models are used in radiobiology to estimate cancer risks and latency periods (time from exposure to clinical cancer). Steps such as initiation, promotion and transformation have been modeled in detail. However, progression, a later step during which malignant cells can develop into clinical symptomatic cancer, has often been approximated simply as a fixed lag time. This approach discounts important stochastic mechanisms in progression and evidence on the high prevalence of dormant tumors. Modeling progression more accurately is therefore important for risk assessment. Unlike models of earlier steps, progression models can readily utilize not only experimental and epidemiological data but also clinical data such as the results of modern screening and imaging. Here, a stochastic progression model is presented. We describe, with minimal parameterization: the initial growth or extinction of a malignant clone after formation of a malignant cell; the likely dormancy caused, for example, by nutrient and oxygen deprivation; and possible escape from dormancy resulting in a clinical cancer. It is shown, using cohort simulations with parameters appropriate for lung adenocarcinomas, that incorporating such processes can dramatically lengthen predicted latency periods. Such long latency periods together with data on timing of radiation-induced cancers suggest that radiation may influence progression itself.
Figures
Similar articles
-
Stochastic population dynamic effects for lung cancer progression.Radiat Res. 2009 Sep;172(3):383-93. doi: 10.1667/RR1621.1. Radiat Res. 2009. PMID: 19708787
-
Analysis of the incidence of solid cancer among atomic bomb survivors using a two-stage model of carcinogenesis.Radiat Res. 1997 Oct;148(4):348-58. Radiat Res. 1997. PMID: 9339951
-
Biologically based analysis of lung cancer incidence in a large Canadian occupational cohort with low-dose ionizing radiation exposure, and comparison with Japanese atomic bomb survivors.J Toxicol Environ Health A. 2006 Jun;69(11):1013-38. doi: 10.1080/00397910500360202. J Toxicol Environ Health A. 2006. PMID: 16840251
-
A diversity of responses displayed by a stochastic model of radiation carcinogenesis allowing for cell death.Math Biosci. 1996 Feb;132(1):1-33. doi: 10.1016/0025-5564(95)00047-x. Math Biosci. 1996. PMID: 8924720 Review.
-
Systems biological and mechanistic modelling of radiation-induced cancer.Radiat Environ Biophys. 2008 Feb;47(1):39-47. doi: 10.1007/s00411-007-0150-z. Epub 2007 Dec 21. Radiat Environ Biophys. 2008. PMID: 18097677 Free PMC article. Review.
Cited by
-
Longitudinal multistage model for lung cancer incidence, mortality, and CT detected indolent and aggressive cancers.Math Biosci. 2012 Nov;240(1):20-34. doi: 10.1016/j.mbs.2012.05.008. Epub 2012 Jun 15. Math Biosci. 2012. PMID: 22705252 Free PMC article.
-
Hypothermia activates adipose tissue to promote malignant lung cancer progression.PLoS One. 2013 Aug 27;8(8):e72044. doi: 10.1371/journal.pone.0072044. eCollection 2013. PLoS One. 2013. PMID: 24015203 Free PMC article.
-
Impact of tumor progression on cancer incidence curves.Cancer Res. 2013 Feb 1;73(3):1086-96. doi: 10.1158/0008-5472.CAN-12-2198. Epub 2012 Oct 10. Cancer Res. 2013. PMID: 23054397 Free PMC article.
-
Late health effects of ionizing radiation: bridging the experimental and epidemiological divide.Radiat Environ Biophys. 2010 May;49(2):109-10. doi: 10.1007/s00411-010-0273-5. Epub 2010 Mar 6. Radiat Environ Biophys. 2010. PMID: 20213137 No abstract available.
-
Repopulation of interacting tumor cells during fractionated radiotherapy: stochastic modeling of the tumor control probability.Med Phys. 2013 Dec;40(12):121716. doi: 10.1118/1.4829495. Med Phys. 2013. PMID: 24320502 Free PMC article.
References
-
- Adam JA, Maggelakis SA. Diffusion regulated growth characteristics of a spherical prevascular carcinoma. Bull Math Biol. 1990;52:549–582. - PubMed
