

Collagen scaffold supplementation does not improve the functional properties of the repaired anterior cruciate ligament
- PMID: 20058276
- PMCID: PMC2858260
- DOI: 10.1002/jor.21071
Collagen scaffold supplementation does not improve the functional properties of the repaired anterior cruciate ligament
Abstract
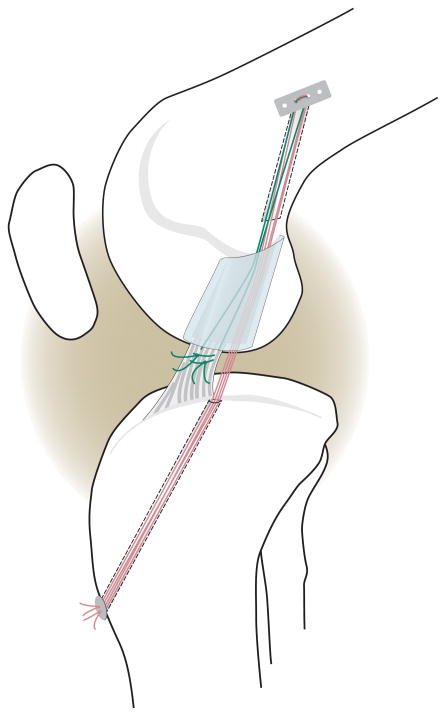
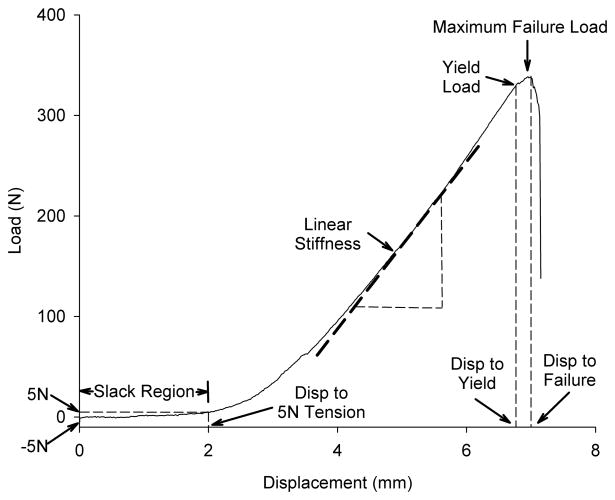
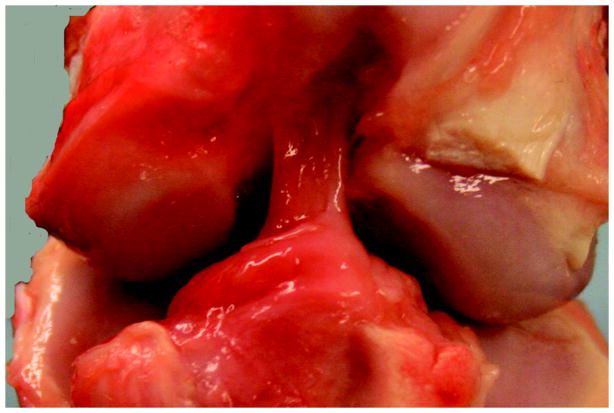
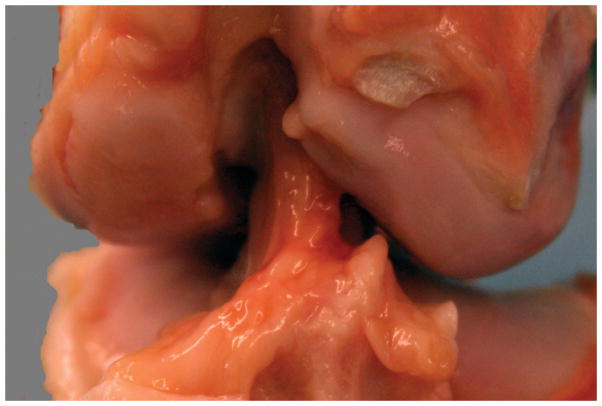
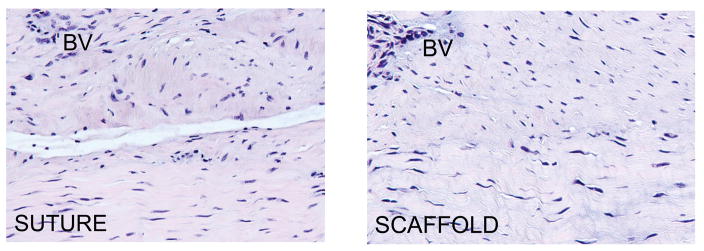
Primary suture anterior cruciate ligament (ACL) repair was abandoned in favor of reconstruction due to a high rate of clinical failures. However, the insertion of a collagen scaffold loaded with platelets into the wound at the time of suture repair ("enhanced primary repair") has been shown to improve functional healing in animal models. Our objectives were to determine if using a collagen scaffold alone (without platelets) would be sufficient to increase the structural properties of the repaired ACL and decrease postoperative knee laxity compared to suture repair without the scaffold. Eight Yucatan minipigs underwent bilateral ACL transection and suture repair. In one knee, the repair was augmented with a collagen scaffold (SCAFFOLD group) while the other had suture alone (SUTURE group). After 13 weeks of healing, knee joint laxity and the structural properties of the ACL were measured. The addition of the collagen scaffold to suture repair of a transected ACL did not significantly improve the mean anteroposterior knee laxity [SCAFFOLD vs. SUTURE: 6.1 +/- 1.4 vs. 4.4 +/- 2.0 mm (p = 0.07), 8.1 +/- 2.0 vs. 7.6 +/- 2.0 mm (p = 0.66), and 6.2 +/- 1.2 vs. 6.1 +/- 1.8 mm (p = 0.85) at 30 degrees, 60 degrees, and 90 degrees flexion, respectively]. Likewise, there were no significant differences in the structural properties [SCAFFOLD vs. SUTURE: 367 +/- 185.9 vs. 322 +/- 122.0N (p = 0.66) and 90.7 +/- 29.5 vs. 85.0 +/- 30.3N/mm (p = 0.74) for the yield load and linear stiffness, respectively]. The use of a collagen scaffold alone to enhance suture repair of the ACL was ineffective in this animal model. Future work will be directed at stimulating biological activity in the scaffold.
(c) 2010 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
Figures
References
-
- Praemer A, Furner S, Rice DP. Musculoskeletal Conditions in the United States. American Academy of Orthopaedic Surgeons 1999
-
- Adriani E, Mariani PP, Maresca G, Santori N. Healing of the patellar tendon after harvesting of its mid-third for anterior cruciate ligament reconstruction and evolution of the unclosed donor site defect. Knee Surg Sports Traumatol Arthrosc. 1995;3:138–143. - PubMed
-
- Cabaud HE, Rodkey WG, Feagin JA. Experimental studies of acute anterior cruciate ligament injury and repair. Am J Sports Med. 1979;7:18–22. - PubMed
-
- O’Donoghue DH, Rockwood C, Frank GR, Jack SC, Kenyon R. Repair of the anterior cruciate ligament in dogs. J Bone Joint Surg [Am] 1966;48:503–519. - PubMed
-
- O’Donoghue DH, Frank GR, Jeter GL, Johnson W, Zeiders JW, Kenyon R. Repair and reconstruction of the anterior cruciate ligament in dogs. Factors influencing long-term results. J Bone Joint Surg [Am] 1971;53:710–718. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
