

Modulatory effects of 5Hz rTMS over the primary somatosensory cortex in focal dystonia--an fMRI-TMS study
- PMID: 20058321
- PMCID: PMC2929458
- DOI: 10.1002/mds.22825
Modulatory effects of 5Hz rTMS over the primary somatosensory cortex in focal dystonia--an fMRI-TMS study
Abstract
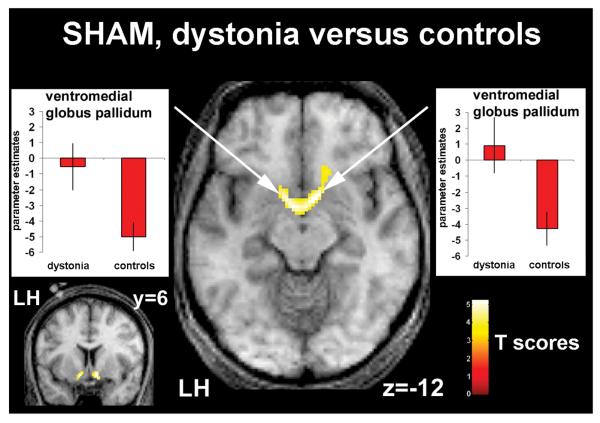
Dystonia is associated with impaired somatosensory ability. The electrophysiological method of repetitive transcranial magnetic stimulation (rTMS) can be used for noninvasive stimulation of the human cortex and can alter cortical excitability and associated behavior. Among others, rTMS can alter/improve somatosensory discrimation abilities, as shown in healthy controls. We applied 5Hz-rTMS over the left primary somatosensory cortex (S1) in 5 patients with right-sided writer's dystonia and 5 controls. We studied rTMS effects on tactile discrimination accuracy and concomitant rTMS-induced changes in hemodynamic activity measured by functional magnetic resonance imaging (fMRI). Before rTMS, patients performed worse on the discrimination task than controls even though fMRI showed greater task-related activation bilaterally in the basal ganglia (BG). In controls, rTMS led to improved discrimination; fMRI revealed this was associated with increased activity of the stimulated S1, bilateral premotor cortex and BG. In dystonia patients, rTMS had no effect on discrimination; fMRI showed similar cortical effects to controls except for no effects in BG. Improved discrimination after rTMS in controls is linked to enhanced activation of S1 and BG. Failure of rTMS to increase BG activation in dystonia may be associated with the lack of effect on sensory discrimination in this group and may reflect impaired processing in BG-S1 connections. Alternatively, the increased BG activation seen in the baseline state without rTMS may reflect a compensatory strategy that saturates a BG contribution to this task.
Figures





Similar articles
-
Motor network reorganization associated with rTMS-induced writing improvement in writer's cramp dystonia.Brain Stimul. 2025 Mar-Apr;18(2):198-210. doi: 10.1016/j.brs.2025.02.005. Epub 2025 Feb 7. Brain Stimul. 2025. PMID: 39924101
-
Repetitive TMS of the somatosensory cortex improves writer's cramp and enhances cortical activity.Neuro Endocrinol Lett. 2010;31(1):73-86. Neuro Endocrinol Lett. 2010. PMID: 20150883 Clinical Trial.
-
Inhibitory rTMS applied on somatosensory cortex in Wilson's disease patients with hand dystonia.J Neural Transm (Vienna). 2017 Oct;124(10):1161-1170. doi: 10.1007/s00702-017-1756-1. Epub 2017 Jul 8. J Neural Transm (Vienna). 2017. PMID: 28689295 Clinical Trial.
-
Contribution of TMS and rTMS in the Understanding of the Pathophysiology and in the Treatment of Dystonia.Front Neural Circuits. 2016 Nov 10;10:90. doi: 10.3389/fncir.2016.00090. eCollection 2016. Front Neural Circuits. 2016. PMID: 27891079 Free PMC article. Review.
-
Exploring the connections between basal ganglia and cortex revealed by transcranial magnetic stimulation, evoked potential and deep brain stimulation in dystonia.Eur J Paediatr Neurol. 2022 Jan;36:69-77. doi: 10.1016/j.ejpn.2021.12.004. Epub 2021 Dec 10. Eur J Paediatr Neurol. 2022. PMID: 34922163 Review.
Cited by
-
Resting-state fMRI study of brain activation using low-intensity repetitive transcranial magnetic stimulation in rats.Sci Rep. 2018 Apr 30;8(1):6706. doi: 10.1038/s41598-018-24951-6. Sci Rep. 2018. PMID: 29712947 Free PMC article.
-
Theta-burst stimulation-induced plasticity over primary somatosensory cortex changes somatosensory temporal discrimination in healthy humans.PLoS One. 2012;7(3):e32979. doi: 10.1371/journal.pone.0032979. Epub 2012 Mar 7. PLoS One. 2012. PMID: 22412964 Free PMC article.
-
Focal dystonia and the Sensory-Motor Integrative Loop for Enacting (SMILE).Front Hum Neurosci. 2014 Jun 20;8:458. doi: 10.3389/fnhum.2014.00458. eCollection 2014. Front Hum Neurosci. 2014. PMID: 24999327 Free PMC article. Review.
-
The functional neuroanatomy of dystonia.Neurobiol Dis. 2011 May;42(2):185-201. doi: 10.1016/j.nbd.2011.01.026. Epub 2011 Feb 12. Neurobiol Dis. 2011. PMID: 21303695 Free PMC article. Review.
-
Applications of Transcranial Magnetic Stimulation for Understanding and Treating Dystonia.Adv Neurobiol. 2023;31:119-139. doi: 10.1007/978-3-031-26220-3_7. Adv Neurobiol. 2023. PMID: 37338699 Review.
References
-
- Bhatia KP, Marsden CD. The behavioural and motor consequences of focal lesions of the basal ganglia in man. Brain. 1994;117(Pt 4):859–876. - PubMed
-
- Hallett M. Pathophysiology of dystonia. J Neural Transm Suppl. 2006:485–488. - PubMed
-
- Mink JW. The basal ganglia: focused selection and inhibition of competing motor programs. Prog Neurobiol. 1996;50:381–425. - PubMed
-
- Sohn YH, Hallett M. Disturbed surround inhibition in focal hand dystonia. Ann Neurol. 2004;56:595–599. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
