

Immunotherapy of cancer: key findings and commentary on the third Tegernsee conference
- PMID: 20061401
- PMCID: PMC3227889
- DOI: 10.1634/theoncologist.2009-0213
Immunotherapy of cancer: key findings and commentary on the third Tegernsee conference
Abstract
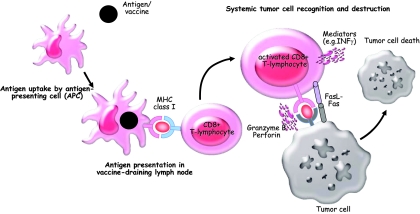
Cancer immunotherapy broadly includes active immunization, as in the use of cancer vaccines, passive immunization, such as the use of adoptive cell therapy and antibodies that modulate tumor function, and immunostimulation, using antibodies and small molecules to treat malignancy by activating or unleashing an endogenous immune response against tumor cells. Currently, >100 different monoclonal antibodies are in use or under evaluation for use as therapeutic agents in various malignancies. Active stimulation of the host's immune system holds promise for achieving durable remission of malignant disease and represents a nontoxic method of therapy if tumor-specific effector cells can be selectively targeted. However, no active-specific treatment strategy (i.e., a therapeutic cancer vaccine) has yet found its way into the clinical armamentarium, although several promising recent reports suggest that, for follicular lymphoma, prostate cancer, and melanoma, clinical benefit was shown for the first time in randomized trials with a vaccine approach. Here, we report on the key findings of the Third Tegernsee Conference on Immunotherapy of Cancer (Feldafing, Germany, July 2-4, 2009) and provide short commentaries on data presented at this meeting regarding the future role of cancer vaccines, recent developments in adoptive cellular therapy, ways to improve immunotherapeutic treatment modalities (e.g., by manipulating the tumor microenvironment), and some novel targeted therapies that are well advanced in clinical testing, all of which have implications for future oncology practice.
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the independent peer reviewers.
Figures
Similar articles
-
Addressing cancer immunotherapy research in Iran: adoptive cell therapy on the horizon.Cytotherapy. 2018 Oct;20(10):1227-1237. doi: 10.1016/j.jcyt.2018.08.002. Epub 2018 Sep 26. Cytotherapy. 2018. PMID: 30266521 Review.
-
Cancer immunotherapy.Biotechnol J. 2006 Feb;1(2):138-47. doi: 10.1002/biot.200500044. Biotechnol J. 2006. PMID: 16892244 Review.
-
Immunotherapy: on the edge between experimental and clinical oncology.J Chemother. 2001 Feb;13(1):15-23. doi: 10.1179/joc.2001.13.1.15. J Chemother. 2001. PMID: 11233795 Review.
-
Prostate cancer vaccines: current status.Semin Oncol. 1999 Apr;26(2):192-201. Semin Oncol. 1999. PMID: 10597730 Review.
-
An overview of cancer immunotherapeutic strategies.Immunotherapy. 2018 Aug;10(11):999-1010. doi: 10.2217/imt-2018-0002. Immunotherapy. 2018. PMID: 30149763 Review.
Cited by
-
Molecular markers to predict clinical outcome and radiation induced toxicity in lung cancer.J Thorac Dis. 2014 Apr;6(4):387-98. doi: 10.3978/j.issn.2072-1439.2013.12.04. J Thorac Dis. 2014. PMID: 24688783 Free PMC article. Review.
-
Ten years of progress in vaccination against cancer: the need to counteract cancer evasion by dual targeting in future therapies.Cancer Immunol Immunother. 2011 Aug;60(8):1127-35. doi: 10.1007/s00262-011-0985-7. Epub 2011 Apr 9. Cancer Immunol Immunother. 2011. PMID: 21479639 Free PMC article. Review.
-
New insights into the role of the immune microenvironment in breast carcinoma.Clin Dev Immunol. 2013;2013:785317. doi: 10.1155/2013/785317. Epub 2013 Jun 3. Clin Dev Immunol. 2013. PMID: 23861693 Free PMC article. Review.
-
Active-specific immunotherapy for non-small cell lung cancer.J Thorac Dis. 2011 Jun;3(2):105-14. doi: 10.3978/j.issn.2072-1439.2010.12.06. J Thorac Dis. 2011. PMID: 22263073 Free PMC article.
-
Simultaneous TLR2 inhibition and TLR9 activation synergistically suppress tumor metastasis in mice.Acta Pharmacol Sin. 2012 Apr;33(4):503-12. doi: 10.1038/aps.2011.193. Epub 2012 Mar 19. Acta Pharmacol Sin. 2012. PMID: 22426694 Free PMC article.
References
-
- Peeters M, Price T, Van Laethem JL. Anti-epidermal growth factor receptor monotherapy in the treatment of metastatic colorectal cancer: Where are we today? The Oncologist. 2009;14:29–39. - PubMed
-
- Wheatly-Price P, Shepherd FA. Targeting angiogenesis in the treatment of lung cancer. J Thorac Oncol. 2008;3:1173–1184. - PubMed
-
- Ross JS, Slodkowska EA, Symmans WF, et al. The HER-2 receptor and breast cancer: Ten years of targeted anti-HER-2 therapy and personalized medicine. The Oncologist. 2009;14:320–368. - PubMed
-
- Ruter J, Barnett BG, Kryczek I, et al. Altering regulatory T cell function in cancer immunotherapy: A novel means to boost the efficacy of cancer vaccines. Front Biosci. 2009;14:1761–1770. - PubMed
-
- Korman A, Yellin M, Keler T. Tumor immunotherapy: Preclinical and clinical activity of anti-CTLA4 antibodies. Curr Opin Investig Drugs. 2005;6:582–591. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
