

Early acute kidney injury predicts progressive renal dysfunction and higher mortality in severely burned adults
- PMID: 20061841
- PMCID: PMC3045668
- DOI: 10.1097/BCR.0b013e3181cb8c87
Early acute kidney injury predicts progressive renal dysfunction and higher mortality in severely burned adults
Abstract
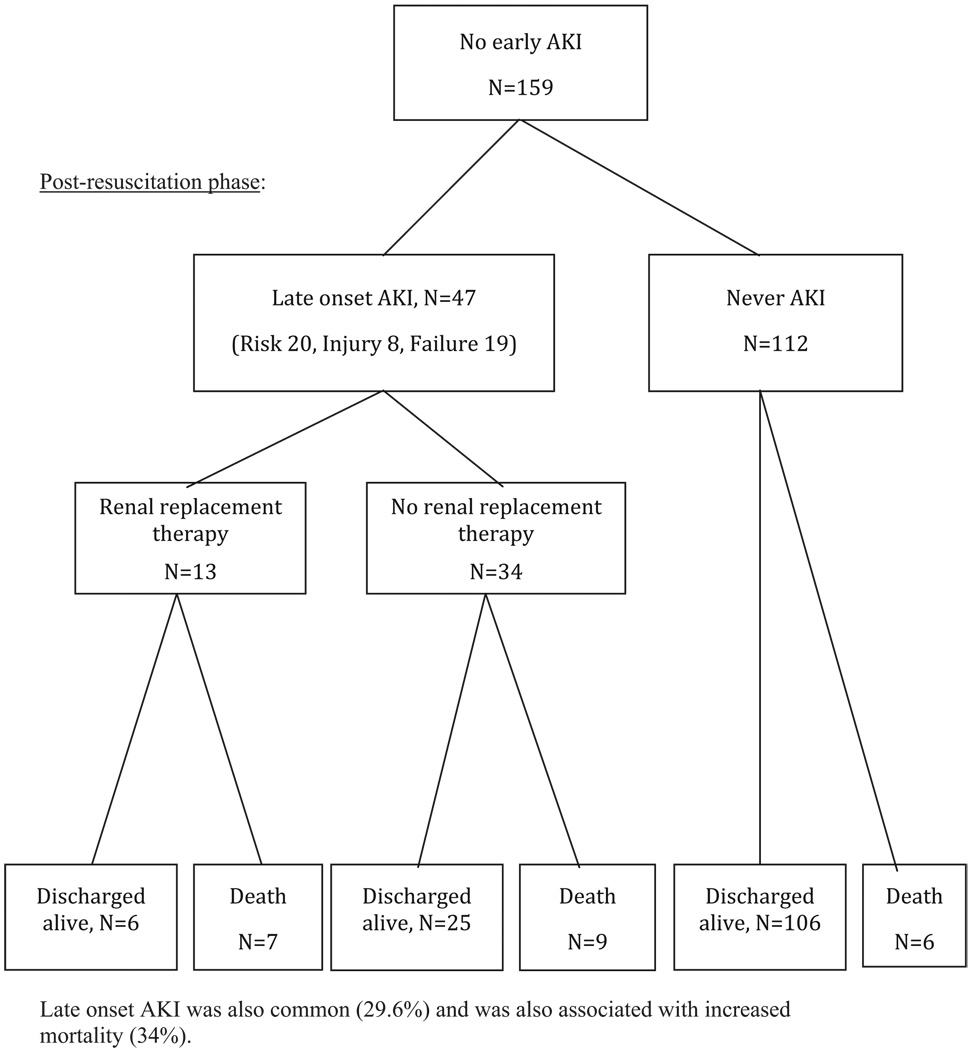
The incidence and prognosis of acute kidney injury (AKI) developing during acute resuscitation have not been well characterized in burn patients. The recently developed Risk, Injury, Failure, Loss, and End-stage (RIFLE) classification provides a stringent stratification of AKI severity and can allow for the study of AKI after burn injury. We hypothesized that AKI frequently develops early during resuscitation and is associated with poor outcomes in severely burned patients. We conducted a retrospective review of patients enrolled in the prospective observational multicenter study "Inflammation and the Host Response to Injury." A RIFLE score was calculated for all patients at 24 hours and throughout hospitalization. Univariate and multivariate analyses were performed to distinguish the impact of early AKI on progressive renal dysfunction, need for renal replacement therapy, and hospital mortality. A total of 221 adult burn patients were included, with a mean TBSA burn of 42%. Crystalloid resuscitation averaged 5.2 ml/kg/%TBSA, with urine output of 1.0 +/- 0.6 ml/kg/hr at 24 hours. Sixty-two patients met criteria for AKI at 24 hours: 23 patients (10%) classified as risk, 32 patients (15%) as injury, and 7 (3%) as failure. After adjusting for age, TBSA, inhalation injury, and nonrenal Acute Physiology and Chronic Health Evaluation II > or =20, early AKI was associated with an adjusted odds ratio 2.9 for death (95% CI 1.1-7.5, P = .03). In this cohort of severely burned patients, 28% of patients developed AKI during acute resuscitation. AKI was not always transient, with 29% developing progressive renal deterioration by RIFLE criteria. Early AKI was associated with early multiple organ dysfunction and higher mortality risk. Better understanding of how early AKI develops and which patients are at risk for progressive renal dysfunction may lead to improved outcomes.
Figures

References
-
- Mustonen KM, Vuola J. Acute renal failure in intensive care burn patients. J Burn Car Res. 2008;29:227–237. - PubMed
-
- Holm C, Horbrand F, von Donnersmarck GH, Mühlbauer W. Acute renal failure in severely burned patients. Burns. 1999;25:171–178. - PubMed
-
- Bellomo R, Ronocco C, Kellum JA, Mehta RL, Palevsky P. Acute Dialysis Quality Initiative Workgroup. Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–R212. - PMC - PubMed
-
- Ricci Z, Cruz D, Ronco C. The RIFLE criteria and mortality in acute kidney injury: a systematic review. Kidney Int. 2008;73:538–546. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
