

Long-term nephrostomy in an adult male spinal cord injury patient who had normal upper urinary tracts but developed bilateral hydronephrosis following penile sheath drainage: pyeloplasty and balloon dilatation of ureteropelvic junction proved futile: a case report
- PMID: 20062594
- PMCID: PMC2803994
- DOI: 10.1186/1757-1626-2-9335
Long-term nephrostomy in an adult male spinal cord injury patient who had normal upper urinary tracts but developed bilateral hydronephrosis following penile sheath drainage: pyeloplasty and balloon dilatation of ureteropelvic junction proved futile: a case report
Abstract
Introduction: The consequences of spinal cord injury upon urinary bladder are readily recognised by patients and health care professionals, since neuropathic bladder manifests itself as urinary incontinence, or retention of urine. But health care professionals and persons with spinal cord injury may not be conversant with neuropathic dysmotility affecting the ureter and renal pelvis. We report an adult male patient with spinal cord injury, who developed bilateral hydronephrosis after he started managing neuropathic bladder by penile sheath drainage.
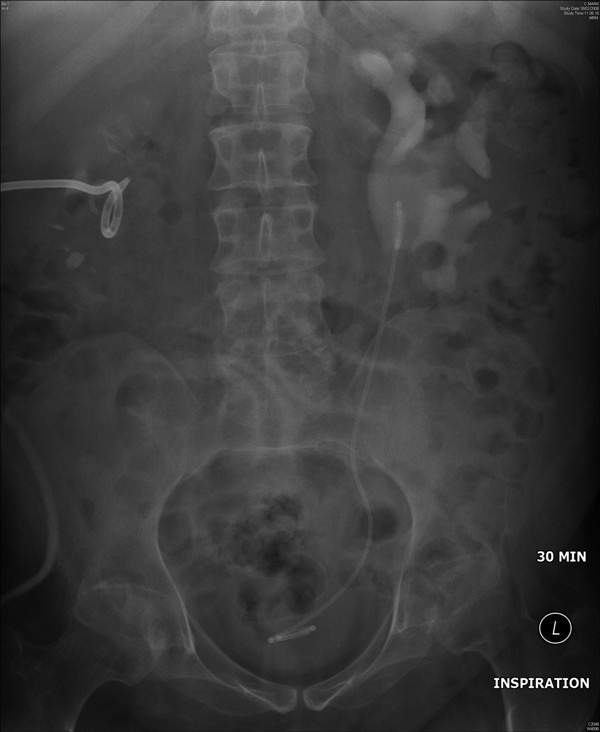
Case presentation: A male patient, born in 1971, sustained spinal cord injury following a motorbike accident in September 1988. In November 1988, intravenous urography showed normal upper tracts. He was advised spontaneous voiding with 2-3 catheterisations a day. In February 1995, this patient developed fever, chills and vomiting. Blood urea: 23.7 mmol/L; creatinine: 334 umol/L. Ultrasound revealed marked hydronephrosis of right kidney and mild hydronephrosis of left kidney. Bilateral nephrostomy was performed in March 1995. Right pyeloplasty was performed in May 1998. In July 2005, this patient developed urine infection and was admitted to a local hospital with fever and rigors. He developed septicaemia and required ventilation. Ultrasound examination of abdomen revealed bilateral hydronephrosis and multiple stones in left kidney. Percutaneous nephrostomy was performed on both sides. Subsequently, extracorporeal shock wave lithotripsy of left renal calculi was carried out. Right nephrostomy tube slipped out in January 2006; percutaneous nephrostomy was performed again. In June 2006, left ureteric antegrade stenting was performed and nephrostomy tube was removed. Currently, right kidney is drained by percutaneous nephrostomy and left kidney is drained by ureteric stent. This patient has indwelling urethral catheter.
Conclusion: It is possible that regular intermittent catheterisations along with anticholinergic medication right from the time of rehabilitation after this patient sustained paraplegia might have prevented the series of urological complications. Key components to successful management of external drainage of kidney in this patient are: [1] use of size 14 French pigtail catheter for long-term nephrostomy, [2] anchoring the catheter to skin to with Percufix catheter cuff to prevent accidental tug [3], replacing the nephrostomy dressing once a week by the same team in order to provide continuity of care, and [4] changing nephrostomy catheter every six months by a senior radiologist.
Figures




Similar articles
-
Recurrent bilateral renal calculi in a tetraplegic patient.Spinal Cord. 1998 Jul;36(7):454-62. doi: 10.1038/sj.sc.3100677. Spinal Cord. 1998. PMID: 9670380
-
Ureteric stents vs percutaneous nephrostomy for initial urinary drainage in children with obstructive anuria and acute renal failure due to ureteric calculi: a prospective, randomised study.BJU Int. 2015 Mar;115(3):473-9. doi: 10.1111/bju.12768. Epub 2014 Oct 20. BJU Int. 2015. PMID: 24698195 Clinical Trial.
-
Hydronephrosis and renal failure following inadequate management of neuropathic bladder in a patient with spinal cord injury: Case report of a preventable complication.Patient Saf Surg. 2012 Sep 26;6(1):22. doi: 10.1186/1754-9493-6-22. Patient Saf Surg. 2012. PMID: 23014062 Free PMC article.
-
[Multiple endoscopy for the treatment of upper urinary tract calculi following ileal conduit: a case report and literature review].Beijing Da Xue Xue Bao Yi Xue Ban. 2017 Aug 18;49(4):733-735. Beijing Da Xue Xue Bao Yi Xue Ban. 2017. PMID: 28816298 Review. Chinese.
-
Treatment of Renal Fungal Ball with Fluconazole Instillation Through a Nephrostomy Tube: Case Report and Literature Review.Am J Case Rep. 2018 Oct 4;19:1179-1183. doi: 10.12659/AJCR.911113. Am J Case Rep. 2018. PMID: 30282963 Free PMC article. Review.
References
-
- Santicioli P, Maggi CA. Myogenic and Neurogenic Factors in the Control of Pyeloureteral Motility and Ureteral Peristalsis. Phamacol Rev. 1998;50(4):683–722. - PubMed
-
- Schmidbauer J, Kratzik C, Klingler HC, Remzi M, Lackner J, Marberger M. Nephrovesical subcutaneous ureteric bypass: long-term results in patients with advanced metastatic disease-improvement of renal function and quality of life. Eur Urol. 2006;50(5):1073–1078. doi: 10.1016/j.eururo.2006.02.025. - DOI - PubMed
LinkOut - more resources
Full Text Sources
