

Homonymous hemianopsia as the leading symptom of a tumor like demyelinating lesion: a case report
- PMID: 20062611
- PMCID: PMC2804011
- DOI: 10.1186/1757-1626-2-9366
Homonymous hemianopsia as the leading symptom of a tumor like demyelinating lesion: a case report
Abstract
Introduction: Differential diagnosis of a cerebral lesion can prove to be a very challenging task for the treating physician. Many non-neoplastic neurological diseases can mimic brain neoplasms on neuroimaging.
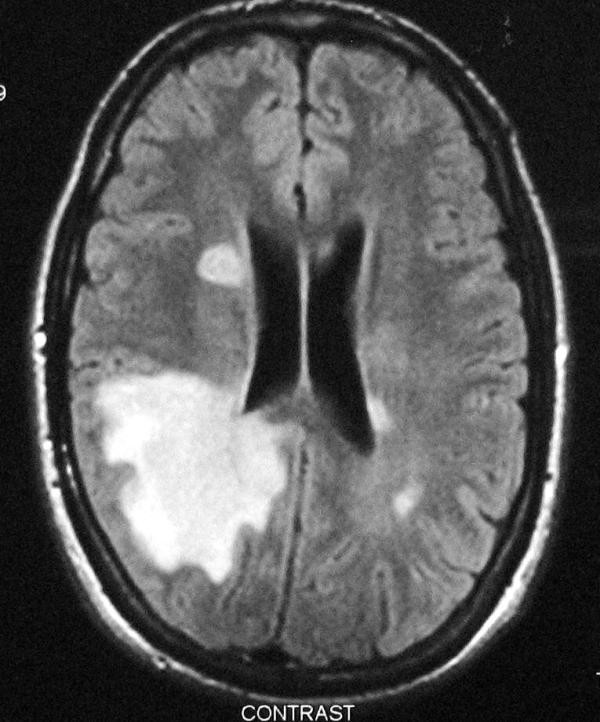
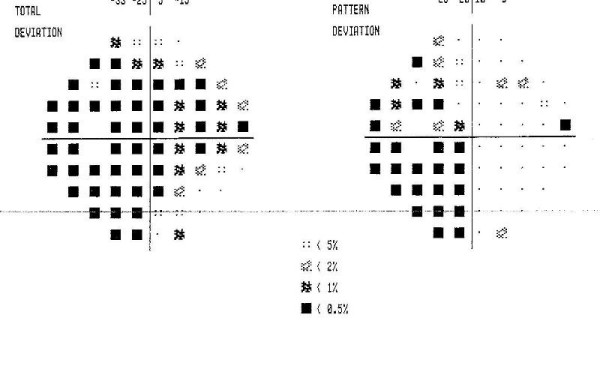
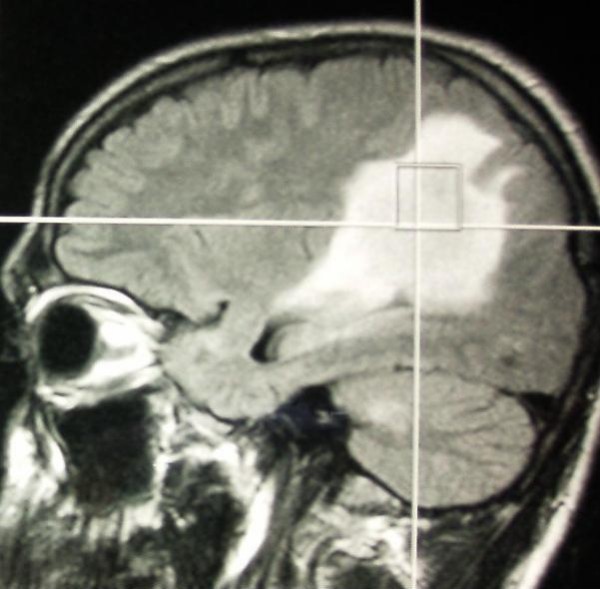
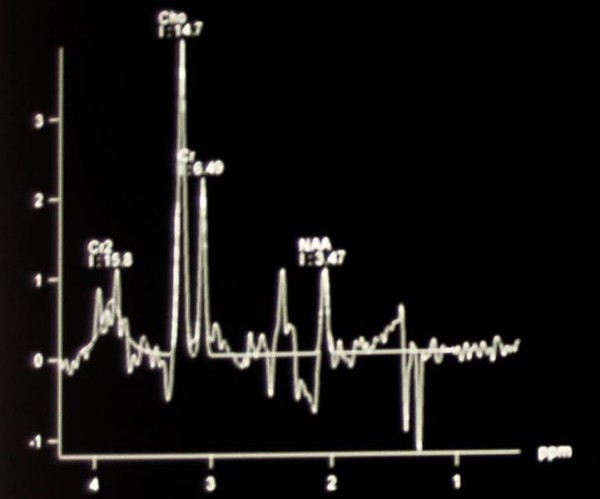
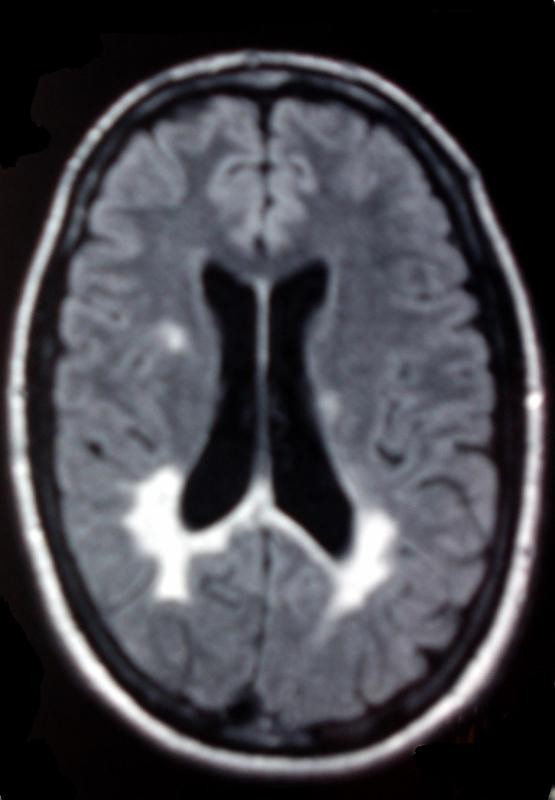
Case presentation: A previously healthy 23-year-old male, presented with blurred vision to the Emergency Department of our Hospital. After initial clinical and serological examination, he was admitted to our clinic for further investigation. Neurological examination showed left homonymous hemianopsia. Brain MRI revealed edema of the right parietal lobe, compressing the posterior region of the right ventricle. Serum viral, immunological and paraneoplasmatic testing were negative. Spectroscopic MRI described the lesions as tumefactive demyelinated plaques. After treating the patient with intravenous corticosteroids, his symptoms rapidly improved and the extensive lesion of the parietal lobe decreased.
Conclusion: In case of young patients with tumor-like lesions, demyelination should always be considered in the differential diagnosis.
Figures

Similar articles
-
Tumefactive demyelinating lesion: experience with two unusual patients.J Postgrad Med. 2010 Apr-Jun;56(2):146-9. doi: 10.4103/0022-3859.65292. J Postgrad Med. 2010. PMID: 20622396
-
Tumefactive demyelination: an unusual cause of a spontaneously resolving homonymous hemianopia.BMJ Case Rep. 2013 Jun 21;2013:bcr2013009363. doi: 10.1136/bcr-2013-009363. BMJ Case Rep. 2013. PMID: 23813509 Free PMC article.
-
Isolated homonymous hemianopsia due to lateral posterior choroidal artery region infarction: a case report.Clin Neurol Neurosurg. 2009 Oct;111(8):713-6. doi: 10.1016/j.clineuro.2009.07.003. Epub 2009 Aug 3. Clin Neurol Neurosurg. 2009. PMID: 19651472
-
[A case of alien hand syndrome after right posterior cerebral artery territory infarction].Rinsho Shinkeigaku. 2003 Aug;43(8):487-90. Rinsho Shinkeigaku. 2003. PMID: 14658401 Review. Japanese.
-
[Homonymous hemianopsia in brain tumors].Klin Monbl Augenheilkd. 1988 May;192(5):543-50. doi: 10.1055/s-2008-1050175. Klin Monbl Augenheilkd. 1988. PMID: 3043102 Review. German.
Cited by
-
Streptococcus Intermedius: A Mimicker of Brain Metastases and A Potential Pitfall for Radiation Oncologists.Adv Radiat Oncol. 2021 Mar 27;6(4):100689. doi: 10.1016/j.adro.2021.100689. eCollection 2021 Jul-Aug. Adv Radiat Oncol. 2021. PMID: 34409201 Free PMC article. No abstract available.
-
Tumefactive demyelination associated with systemic lupus erythematosus.BMJ Case Rep. 2012 May 11;2012:bcr0220125743. doi: 10.1136/bcr.02.2012.5743. BMJ Case Rep. 2012. PMID: 22605871 Free PMC article.
References
LinkOut - more resources
Full Text Sources
