

Simultaneous sleep study and nasoendoscopic investigation in a patient with obstructive sleep apnoea syndrome refractory to continuous positive airway pressure: a case report
- PMID: 20062744
- PMCID: PMC2803838
- DOI: 10.1186/1752-1947-3-9315
Simultaneous sleep study and nasoendoscopic investigation in a patient with obstructive sleep apnoea syndrome refractory to continuous positive airway pressure: a case report
Abstract
Introduction: The standard treatment for obstructive sleep apnoea syndrome is nasal continuous positive airway pressure. In most cases the obstruction is located at the oropharyngeal level, and nasal continuous positive airway pressure is usually effective. In cases of non-response to nasal continuous positive airway pressure other treatments like mandibular advancement devices or upper airway surgery (especially bi-maxillary advancement) may also be considered.
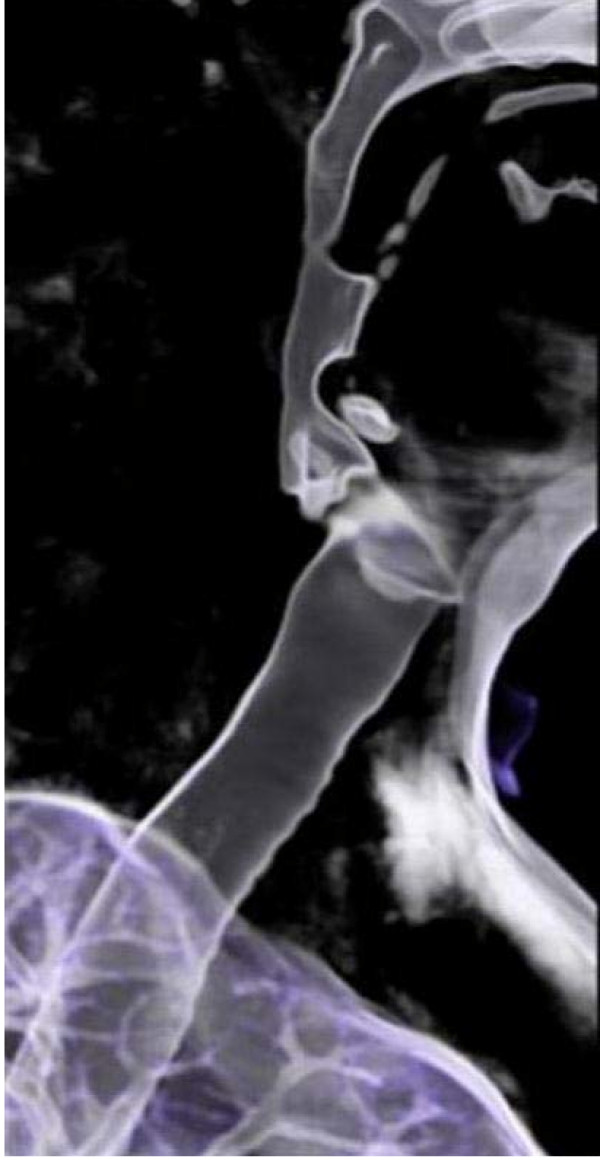
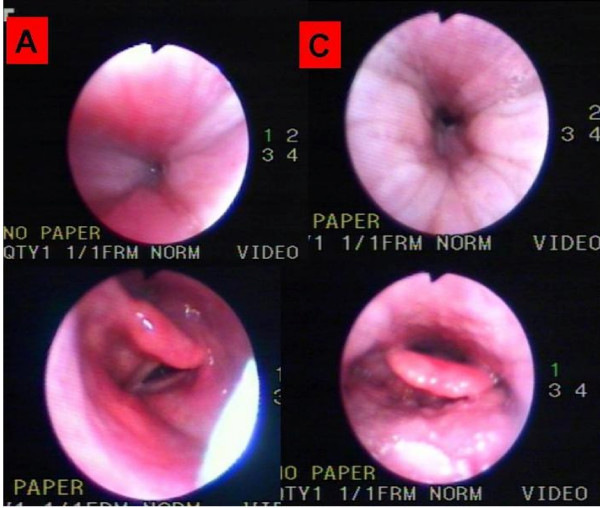
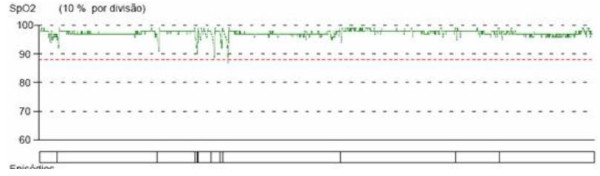
Case presentation: We report the case of a 38-year-old Caucasian man with severe obstructive sleep apnoea syndrome, initially refractory to nasal continuous positive airway pressure (and subsequently also to a mandibular advancement devices), in which the visualization of the upper airway with sleep endoscopy and the concomitant titration of positive pressure were useful in the investigation and resolution of sleep disordered breathing. In fact, there was a marked reduction in the size of his nasopharynx, and a paresis of his left aryepiglotic fold with hypertrophy of the right aryepiglotic fold. The application of bi-level positive airway pressure and an oral interface successfully managed his obstructive sleep apnoea.
Conclusion: This is a rare case of obstructive sleep apnoea syndrome refractory to treatment with nocturnal ventilatory support. Visualization of the endoscopic changes, during sleep and under positive pressure, was of great value to understanding the mechanisms of refractoriness. It also oriented the therapeutic option. Refractoriness to obstructive sleep apnoea therapy with continuous positive airway pressure is rare, and each case should be approached individually.
Figures


Similar articles
-
Never say never: circumventing a contraindication to control apnoea-induced epileptic events with a mandibular advancement device.J Laryngol Otol. 2018 Nov;132(11):1036-1038. doi: 10.1017/S0022215118001858. Epub 2018 Nov 5. J Laryngol Otol. 2018. PMID: 30394239
-
Volumetric three-dimensional computed tomographic evaluation of the upper airway in patients with obstructive sleep apnoea syndrome treated by maxillomandibular advancement.Br J Oral Maxillofac Surg. 2014 Nov;52(9):831-7. doi: 10.1016/j.bjoms.2014.07.101. Epub 2014 Aug 13. Br J Oral Maxillofac Surg. 2014. PMID: 25129655
-
Drug-induced sleep endoscopy as a selection tool for mandibular advancement therapy by oral device in patients with mild to moderate obstructive sleep apnoea.Acta Otorhinolaryngol Ital. 2015 Dec;35(6):426-32. doi: 10.14639/0392-100X-959. Acta Otorhinolaryngol Ital. 2015. PMID: 26900249 Free PMC article.
-
Obstructive sleep apnoea syndrome and its management.Ther Adv Chronic Dis. 2015 Sep;6(5):273-85. doi: 10.1177/2040622315590318. Ther Adv Chronic Dis. 2015. PMID: 26336596 Free PMC article. Review.
-
[Non-CPAP therapies in obstructive sleep apnoea: an overview].Pneumologie. 2013 Jan;67(1):50-7. doi: 10.1055/s-0032-1325903. Epub 2012 Dec 17. Pneumologie. 2013. PMID: 23247597 Review. German.
Cited by
-
[Drug-induced sedation endoscopy-quo vadis? : Review and outlook].HNO. 2017 Feb;65(2):125-133. doi: 10.1007/s00106-016-0329-1. HNO. 2017. PMID: 28116457 Review. German.
References
-
- Van Boxem TJM, de Groot GH. Prevalence and severity of sleep-disordered breathing in a group of morbidly obese patients. Neth J Med. 1999;54(5):202–206. - PubMed
-
- Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, Dágostino RB, Newman AB, Lebowitz MD, Pickering TG. Association of sleep-disordered breathing, sleep Apnoea, and hypertension in a large community-based study: sleep heart health study. JAMA. 2000;283(14):1829–1836. doi: 10.1001/jama.283.14.1829. - DOI - PubMed
LinkOut - more resources
Full Text Sources
