

Severe malaria - a case of fatal Plasmodium knowlesi infection with post-mortem findings: a case report
- PMID: 20064229
- PMCID: PMC2818646
- DOI: 10.1186/1475-2875-9-10
Severe malaria - a case of fatal Plasmodium knowlesi infection with post-mortem findings: a case report
Abstract
Background: Zoonotic malaria caused by Plasmodium knowlesi is an important, but newly recognized, human pathogen. For the first time, post-mortem findings from a fatal case of knowlesi malaria are reported here.
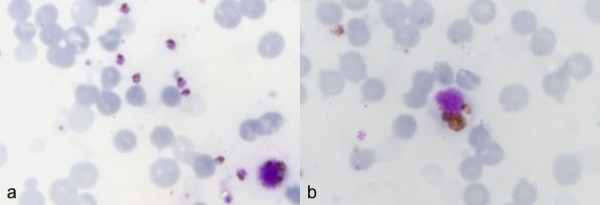
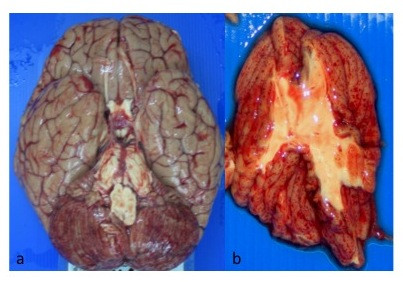
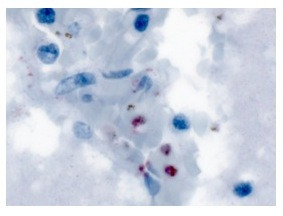
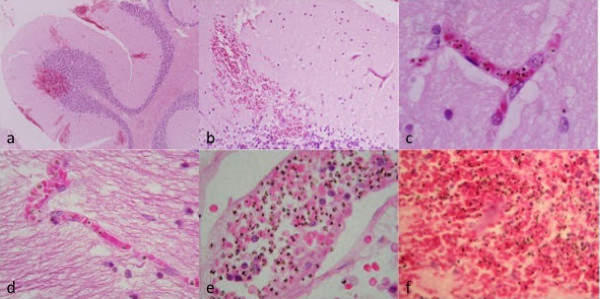
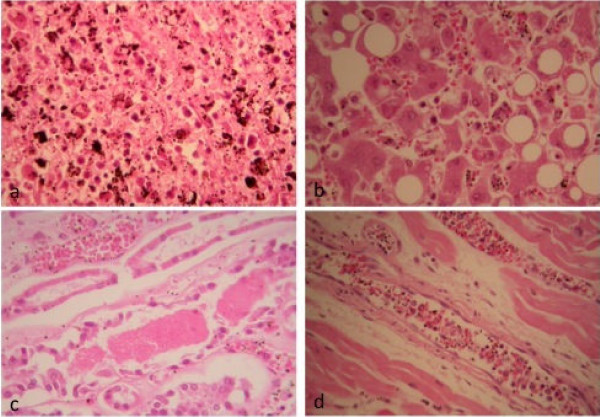
Case presentation: A formerly healthy 40 year-old male became symptomatic 10 days after spending time in the jungle of North Borneo. Four days later, he presented to hospital in a state of collapse and died within two hours. He was hyponatraemic and had elevated blood urea, potassium, lactate dehydrogenase and amino transferase values; he was also thrombocytopenic and eosinophilic. Dengue haemorrhagic shock was suspected and a post-mortem examination performed. Investigations for dengue virus were negative. Blood for malaria parasites indicated hyperparasitaemia and single species P. knowlesi infection was confirmed by nested-PCR. Macroscopic pathology of the brain and endocardium showed multiple petechial haemorrhages, the liver and spleen were enlarged and lungs had features consistent with ARDS. Microscopic pathology showed sequestration of pigmented parasitized red blood cells in the vessels of the cerebrum, cerebellum, heart and kidney without evidence of chronic inflammatory reaction in the brain or any other organ examined. Brain sections were negative for intracellular adhesion molecule-1. The spleen and liver had abundant pigment containing macrophages and parasitized red blood cells. The kidney had evidence of acute tubular necrosis and endothelial cells in heart sections were prominent.
Conclusions: The overall picture in this case was one of systemic malaria infection that fit the WHO classification for severe malaria. Post-mortem findings in this case were unexpectedly similar to those that define fatal falciparum malaria, including cerebral pathology. There were important differences including the absence of coma despite petechial haemorrhages and parasite sequestration in the brain. These results suggest that further study of knowlesi malaria will aid the interpretation of, often conflicting, information on malaria pathophysiology in humans.
Figures
References
-
- World Health Organization, World Malaria Report. 2008.
-
- Coatney GR, Collins WE, Warren M, Contacos PG. The primate malarias. Bethesda, MD: U.S. Department of Health, Education and Welfare, National Institutes of Health; 1971.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
