

Immune and hemorheological changes in chronic fatigue syndrome
- PMID: 20064266
- PMCID: PMC2829521
- DOI: 10.1186/1479-5876-8-1
Immune and hemorheological changes in chronic fatigue syndrome
Abstract
Background: Chronic Fatigue Syndrome (CFS) is a multifactorial disorder that affects various physiological systems including immune and neurological systems. The immune system has been substantially examined in CFS with equivocal results, however, little is known about the role of neutrophils and natural killer (NK) phenotypes in the pathomechanism of this disorder. Additionally the role of erythrocyte rheological characteristics in CFS has not been fully expounded. The objective of this present study was to determine deficiencies in lymphocyte function and erythrocyte rheology in CFS patients.
Methods: Flow cytometric measurements were performed for neutrophil function, lymphocyte numbers, NK phenotypes (CD56(dim)CD16(+) and CD56(bright)CD16(-)) and NK cytotoxic activity. Erythrocyte aggregation, deformability and fibrinogen levels were also assessed.
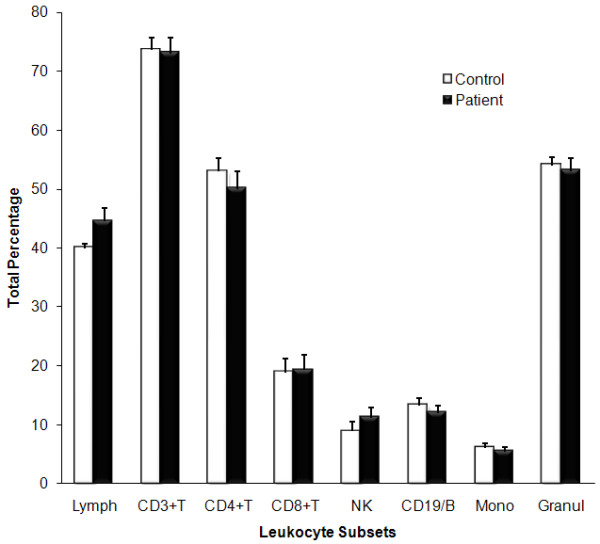
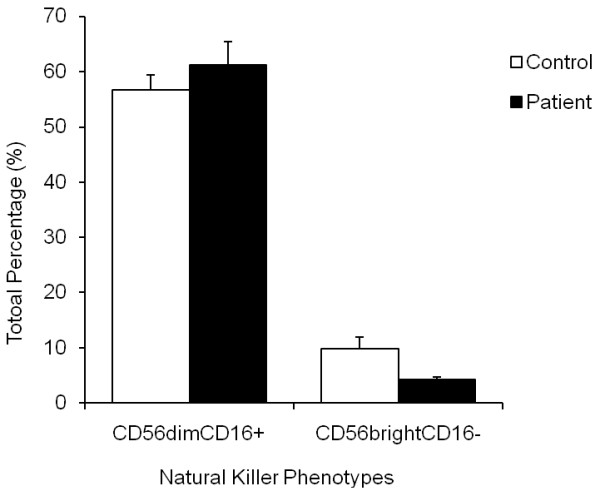
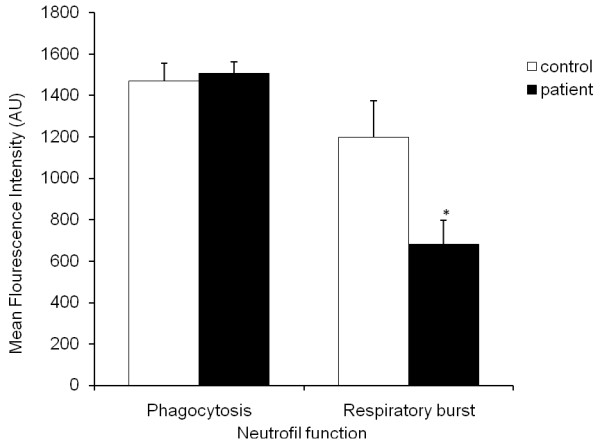
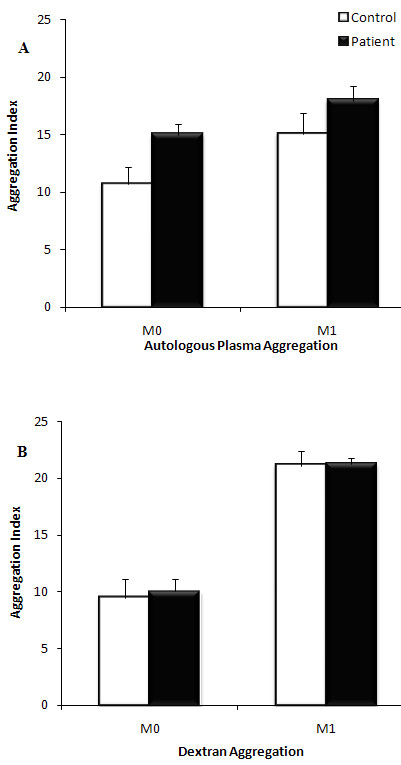
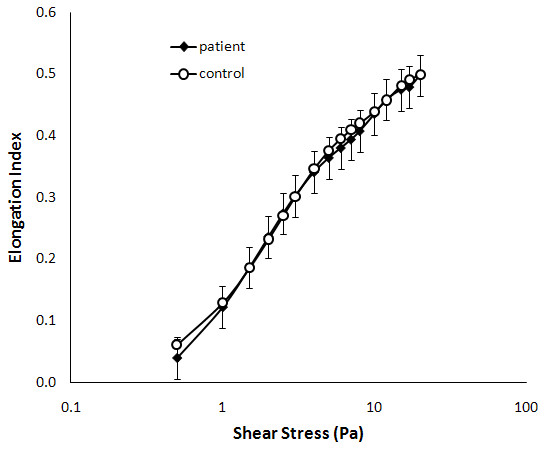
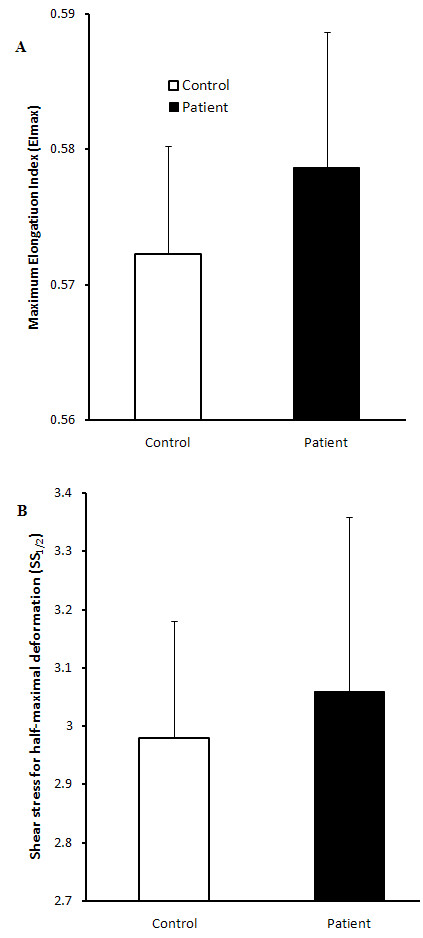
Results: CFS patients (n = 10) had significant decreases in neutrophil respiratory burst, NK cytotoxic activity and CD56(bright)CD16(-) NK phenotypes in comparison to healthy controls (n = 10). However, hemorheological characteristic, aggregation, deformability, fibrinogen, lymphocyte numbers and CD56(dim)CD16(+) NK cells were similar between the two groups.
Conclusion: These results indicate immune dysfunction as potential contributors to the mechanism of CFS, as indicated by decreases in neutrophil respiratory burst, NK cell activity and NK phenotypes. Thus, immune cell function and phenotypes may be important diagnostic markers for CFS. The absence of rheological changes may indicate no abnormalities in erythrocytes of CFS patients.
Figures
References
-
- Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann Intern Med. 1994;121:953–959. - PubMed
-
- Ojo-Amaise EA, Conley EJ, Peters JB. Decreased natural killer cell activity is associated with severity of chronic fatigue syndrome. Clin Infect Dis. 1994;18(Suppl 1):157–159. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
