

The clinical presentations of ectopic biliary drainage into duodenal bulbus and stomach with a thorough review of the current literature
- PMID: 20064279
- PMCID: PMC2881112
- DOI: 10.1186/1471-230X-10-2
The clinical presentations of ectopic biliary drainage into duodenal bulbus and stomach with a thorough review of the current literature
Abstract
Background: Ectopic biliary drainage is a rare congenital anomaly on which we have scarce data in the current literature.
Methods: The data were collected from the records of 400 endoscopic retrograde cholangio-pancreatography (ERCP). In this report, we present 10 cases (male/female: 9/1, mean age 54 years, range 38-74) with ectopic biliary openings into the duodenum and/or stomach diagnosed by endoscopic retrograde cholangio-pancreatography (ERCP).
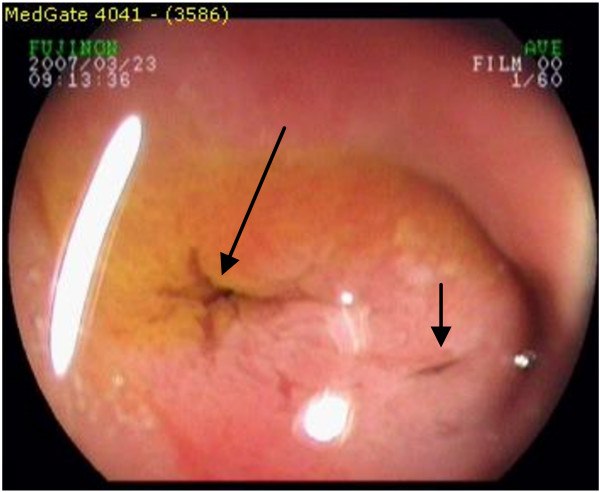
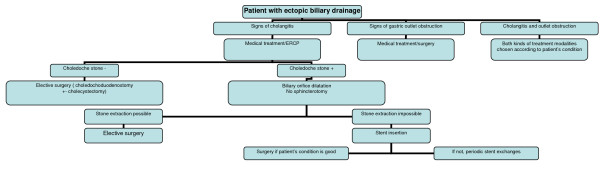
Results: In our series, the frequency of ectopic biliary drainage is 2% (10 out of 400 ERCPs). Recurrent attacks of cholangitis and complicated ulcer formation in the distal stomach and bulbar duodenum were the most common signs in the present series. The sites of ectopic biliary drainage were the stomach in 1 case, the duodenum bulbus in 7 cases and the postbulbar duodenum in 2 cases. Bulbar ulcer, deformed pylorus and bulbus were present in 7 cases, apical bulbar stricture in 2, gastric ulcer in 1, pyloroplasty and/or gastroenterostomy in 3 cases. One case had had previous bleeding episode. Some of them had undergone previous surgeries for gall-stone disease (cholecystectomy in 5 cases, bile duct operation in 3 cases) and ulcer complications (pyloroplasty/gastroenterostomy in 3 cases). ERCP revealed dilatation of the biliary tree and hook shaped distal choledochus in all cases, choledocholithiasis in 7 and Mirizzi syndrome in 1. Endoscopic balloon dilatations for gastric outlet obstruction, extraction of bile stones after balloon dilating the ectopic site, surgery for difficult cases with large bile duct stones or with gastric outlet obstruction were preferred methods in this series of patients.
Conclusion: With this report, we have to remind that ectopic biliary drainage must be considered in the differential diagnosis when the clinician faces cases with gastric outlet obstruction due to peptic ulcer formation accompanied by cholangitis/cholestasis.
Figures







Similar articles
-
Retrospective analysis of cases with an ectopic opening of the common bile duct into duodenal bulb.Adv Clin Exp Med. 2018 Oct;27(10):1361-1364. doi: 10.17219/acem/69691. Adv Clin Exp Med. 2018. PMID: 30062869
-
Ectopic opening of the common bile duct into various sites of the upper digestive tract: a case series.Gastrointest Endosc. 2010 Jul;72(1):198-203. doi: 10.1016/j.gie.2010.02.012. Epub 2010 May 20. Gastrointest Endosc. 2010. PMID: 20493479
-
Anomalous opening of the common bile duct into the duodenal bulb: endoscopic treatment.BMC Gastroenterol. 2007 Jul 5;7:26. doi: 10.1186/1471-230X-7-26. BMC Gastroenterol. 2007. PMID: 17610747 Free PMC article.
-
Management of biliary and duodenal complications of chronic pancreatitis.World J Surg. 2003 Nov;27(11):1258-70. doi: 10.1007/s00268-003-7246-7. Epub 2003 Oct 13. World J Surg. 2003. PMID: 14534824 Review.
-
Laparoscopic exploration of common bile duct in difficult choledocholithiasis.Surg Endosc. 2004 Jun;18(6):910-4. doi: 10.1007/s00464-003-8216-8. Epub 2004 Apr 21. Surg Endosc. 2004. PMID: 15095079 Review.
Cited by
-
Ectopic opening of common bile duct into the duodenal bulb: magnetic resonance cholangiopancreatography findings.Diagn Interv Radiol. 2022 Jul;28(4):286-293. doi: 10.5152/dir.2022.201026. Diagn Interv Radiol. 2022. PMID: 35950273 Free PMC article.
-
Efficacy and safety of therapeutic ERCP in patients with ectopic papilla of Vater.Medicine (Baltimore). 2020 Jan;99(1):e18536. doi: 10.1097/MD.0000000000018536. Medicine (Baltimore). 2020. PMID: 31895789 Free PMC article.
-
Ectopic papilla of Vater in duodenum bulb: A hospital-based study.Medicine (Baltimore). 2019 Feb;98(8):e14642. doi: 10.1097/MD.0000000000014642. Medicine (Baltimore). 2019. PMID: 30813203 Free PMC article.
-
Ectopic opening of the common bile duct into the duodenal bulb with recurrent choledocholithiasis: A case report.World J Clin Cases. 2021 Jul 6;9(19):5332-5338. doi: 10.12998/wjcc.v9.i19.5332. World J Clin Cases. 2021. PMID: 34307586 Free PMC article.
-
A Case of an Ectopic Ampulla of Vater in the Pyloric Channel.ACG Case Rep J. 2014 Apr 4;1(3):161-3. doi: 10.14309/crj.2014.37. eCollection 2014 Apr. ACG Case Rep J. 2014. PMID: 26157861 Free PMC article.
References
-
- Hekimoglu K, Ustundag Y, Saritas U. Ectopic openings of the bilio-pancreatic ducts in the stomach in an elderly case presenting with choledocholithiasis and acute cholangitis. J Gastrointestin Liver Dis. 2008;17:238–9. - PubMed
-
- Doty J, Hassal E, Fonkalsrud EW. Anomalous drainage of the common bile duct into the fourth portion of the duodenum. Arch Surg. 1985;120:1077–9. - PubMed
-
- Koşar Y, Gürkaynak G, Tezel A, Oğuz D, Sahin B. Biliary opening anomalies: ectopic drainage of pancreaticobiliary ducts. Endoscopy. 1998;30:S4–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
