

Defining cerebrospinal fluid white blood cell count reference values in neonates and young infants
- PMID: 20064869
- PMCID: PMC3033868
- DOI: 10.1542/peds.2009-1181
Defining cerebrospinal fluid white blood cell count reference values in neonates and young infants
Abstract
Objective: Cerebrospinal fluid (CSF) white blood cell (WBC) counts for neonates and young infants are usually interpreted on the basis of values reported in reference texts or handbooks; however, current reference texts either present normal CSF parameters without citation or cite studies with significant limitations. The objective of this study was to determine accurate, age-specific reference values for CSF WBC counts in a large population of neonates and young infants.
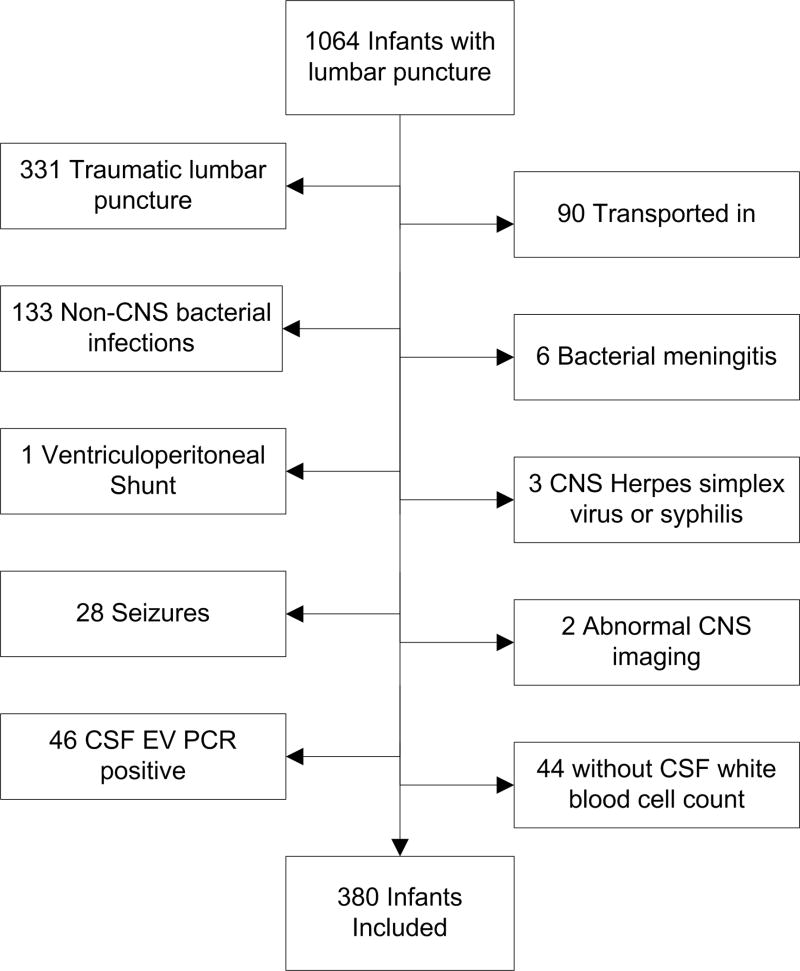
Methods: This cross-sectional study included patients who were aged < or =56 days and had a lumbar puncture performed in the emergency department from January 1, 2005, to June 30, 2007. Patients were excluded from analysis for conditions that are suspected to cause CSF pleocytosis, including traumatic lumbar puncture, serious bacterial infection, congenital infection, seizure, and presence of a ventricular shunt. Children who tested positive for enterovirus (EV) in the CSF by polymerase chain reaction were also excluded. Two-sample Wilcoxon rank-sum tests were used to compare median CSF WBC values of those who had negative EV testing with those who did not have EV testing.
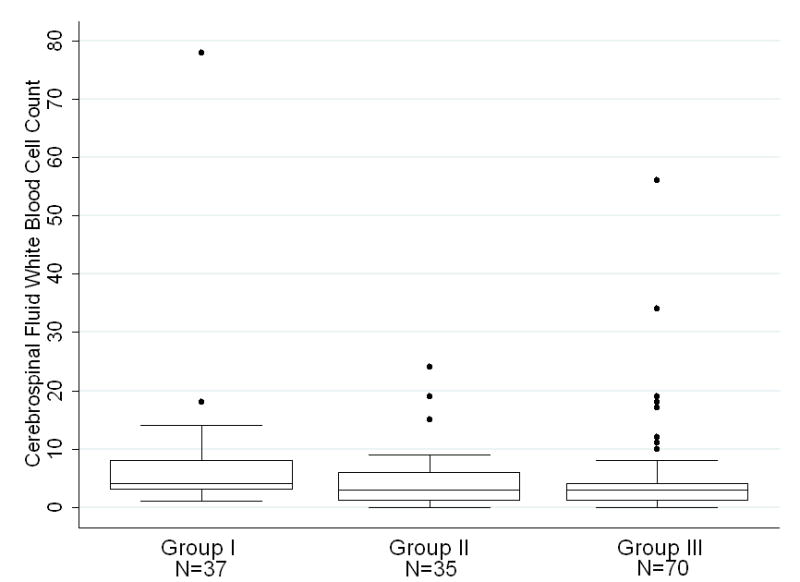
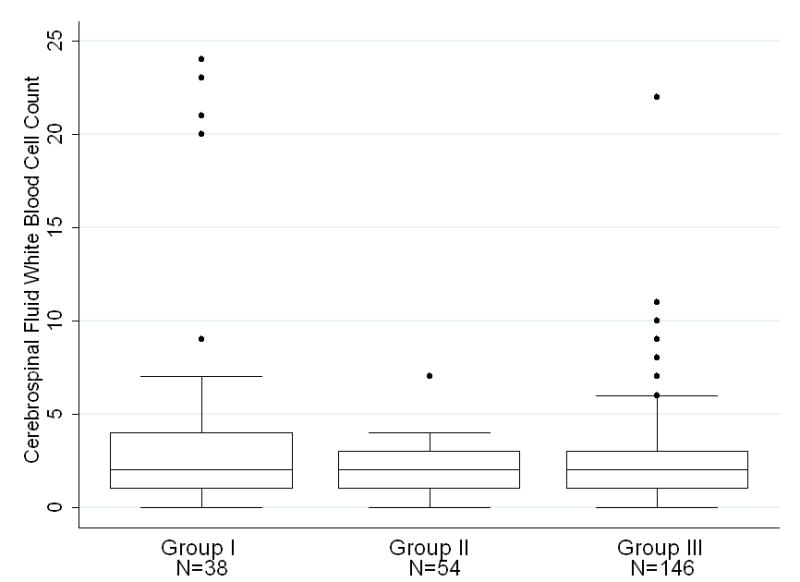
Results: A total of 380 (36%) of 1064 patients met inclusion criteria; 54% were male, 15% were preterm, and 39% presented during EV season. The median CSF WBC count was significantly higher in infants who were aged < or =28 days (3/microL, 95th percentile: 19/microL) than in infants who were aged 29 to 56 days (2/microL, 95th percentile: 9/microL; P < .001). In both age groups, infants with a negative EV PCR had a higher upper bound of the 95% confidence interval of the mean values compared with infants who did not have EV testing performed.
Conclusions: We determined age-specific CSF WBC reference values in a large cohort of neonates and young infants that can be used to interpret accurately the results of lumbar punctures in this population.
Figures
References
-
- Behrman RE, Kliegman R, Jenson HB. Nelson Textbook of Pediatrics. 17. Philadelphia: Saunders; 2004.
-
- McMillan JA, Feigin RD, DeAngelis C, Jones MD. Oski’s pediatrics: principles & practice. 4. Philadelphia: Lippincott Williams & Wilkins; 2006.
-
- Robertson J, Shilkofski N, editors. Johns Hopkins: The Harriet Lane Handbook: A Manual for Pediatric House Officers. 17. Philadelphia: Elsevier Mosby; 2005.
-
- Feigin RD, Cherry JD, Demmler GJ, Kaplan SL. Textbook of Pediatric Infectious Diseases. 5. Philadelphia: Saunders; 2004.
-
- Remington JS, Klein JO. Infectious Diseases of the Fetus and Newborn Infant. 6. Philadelphia: Elsevier Saunders; 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
