

Fundus autofluorescence imaging of the white dot syndromes
- PMID: 20065216
- PMCID: PMC3025103
- DOI: 10.1001/archophthalmol.2009.368
Fundus autofluorescence imaging of the white dot syndromes
Abstract
Objective: To characterize the fundus autofluorescence (FAF) findings in patients with white dot syndromes (WDSs).
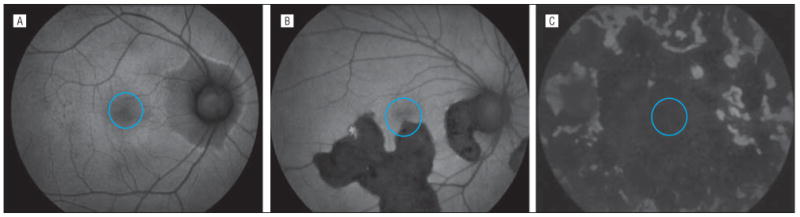
Methods: Patients with WDSs underwent ophthalmic examination, fundus photography, fluorescein angiography, and FAF imaging. Patients were categorized as having no, minimal, or predominant foveal hypoautofluorescence. The severity of visual impairment was then correlated with the degree of foveal hypoautofluorescence.
Results: Fifty-five eyes of 28 patients with WDSs were evaluated. Visual acuities ranged from 20/12.5 to hand motions. Diagnoses included serpiginous choroidopathy (5 patients), birdshot retinochoroidopathy (10), multifocal choroiditis (8), relentless placoid chorioretinitis (1), presumed tuberculosis-associated serpiginouslike choroidopathy (1), acute posterior multifocal placoid pigment epitheliopathy (1), and acute zonal occult outer retinopathy (2). In active serpiginous choroidopathy, notable hyperautofluorescence in active disease distinguished it from the variegated FAF features of tuberculosis-associated serpiginouslike choroidopathy. The percentage of patients with visual acuity impairment of less than 20/40 differed among eyes with no, minimal, and predominant foveal hypoautofluorescence (P < .001). Patients with predominant foveal hypoautofluorescence demonstrated worse visual acuity than those with minimal or no foveal hypoautofluorescence (both P < .001).
Conclusions: Fundus autofluorescence imaging is useful in the evaluation of the WDS. Visual acuity impairment is correlated with foveal hypoautofluorescence. Further studies are needed to evaluate the precise role of FAF imaging in the WDSs.
Figures






Comment in
-
Foveal hypoautofluorescence: does it correlate to visual acuity in white dot syndromes?Arch Ophthalmol. 2010 Dec;128(12):1628-9; author reply 1629-30. doi: 10.1001/archophthalmol.2010.278. Arch Ophthalmol. 2010. PMID: 21149795 No abstract available.
References
-
- Quillen DA, Davis JB, Gottlieb JL, et al. The white dot syndromes. Am J Ophthalmol. 2004;137(3):538–550. - PubMed
-
- Matsumoto Y, Haen SP, Spaide RF. The white dot syndromes. Compr Ophthalmol Update. 2007;8(4):179–200. 203–204. - PubMed
-
- Jones BE, Jampol LM, Yannuzzi LA, et al. Relentless placoid chorioretinitis: a new entity or an unusual variant of serpiginous chorioretinitis? Arch Ophthalmol. 2000;118(7):931–938. - PubMed
-
- Gupta V, Gupta A, Arora S, Bambery P, Dogra MR, Agarwal A. Presumed tubercular serpiginouslike choroiditis: clinical presentations and management. Ophthalmology. 2003;110(9):1744–1749. - PubMed
-
- Gass JD. Acute zonal occult outer retinopathy: Donders Lecture: the Netherlands Ophthalmological Society, Maastricht, Holland, June 19, 1992. J Clin Neuroophthalmol. 1993;13(2):79–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
