

Case Reports
doi: 10.3748/wjg.v16.i2.275.
Single port laparoscopic right hemicolectomy with D3 dissection for advanced colon cancer
Affiliations
- PMID: 20066750
- PMCID: PMC2806569
- DOI: 10.3748/wjg.v16.i2.275
Item in Clipboard
Case Reports
Single port laparoscopic right hemicolectomy with D3 dissection for advanced colon cancer
World J Gastroenterol.
.
Abstract
We report the first case of single port laparoscopic right hemicolectomy for advanced colon cancer. An abdominal 3 cm length incision was made via the umbilicus. A small wound retractor and a surgical glove were used as a single port. All soft tissue anterior to the superior mesenteric vein was completely removed and D3 lymph node dissection was achieved. The total operative time was 180 min with minimal blood loss (< 50 mL). The size of the tumor was 5 cm x 3 cm and its tumor stage was T3N0. Sixty-nine lymph nodes were harvested and none were positive. We believe that single port surgery for colon cancer is a feasible and safe procedure with surgical results comparable to conventional laparoscopic procedures.
Figures
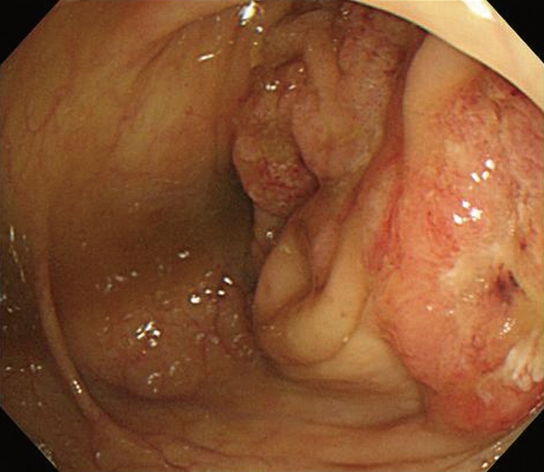
Encircling mass in the ascending colon visualized during colonoscopy.
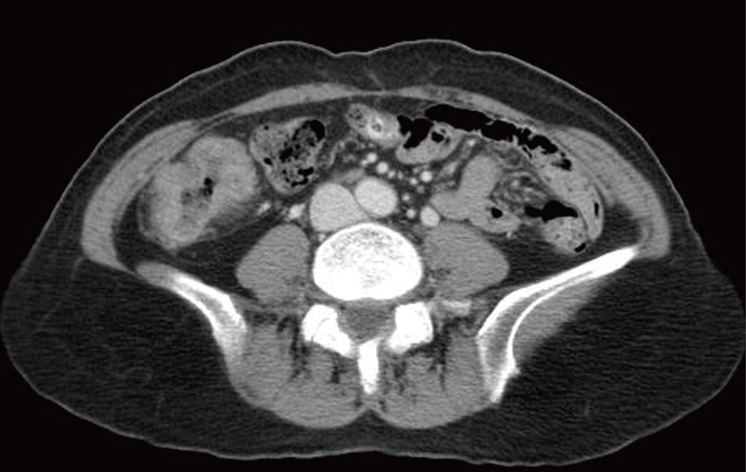
Abdominal CT showed enhanced wall thickening in the ascending colon.

Operative photograph of the single port setting with multiple trocars and instruments.
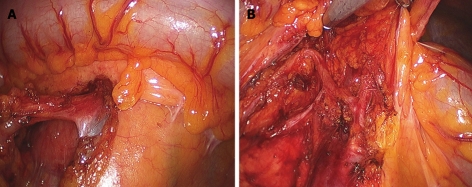
Single port laparoscopic right hemicolectomy with D3 node dissection around the superior mesenteric vein (A) and artery (B).
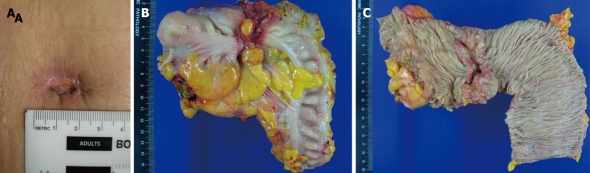
Surgical wound around the umbilicus (A) and surgical specimen of the resected colon (B and C).
Similar articles
-
Robotic Extended Right Hemicolectomy with Complete Mesocolic Excision and D3 Lymph Node Dissection.Ann Surg Oncol. 2019 Nov;26(12):3990-3991. doi: 10.1245/s10434-019-07692-2. Epub 2019 Aug 12. Ann Surg Oncol. 2019. PMID: 31407176 Free PMC article.
-
Variation and treatment of vessels in laparoscopic right hemicolectomy.Surg Endosc. 2018 Mar;32(3):1583-1584. doi: 10.1007/s00464-017-5751-2. Epub 2017 Jul 21. Surg Endosc. 2018. PMID: 28733739
-
Indocyanine Green Fluorescence Imaging-Guided Laparoscopic Surgery Could Achieve Radical D3 Dissection in Patients With Advanced Right-Sided Colon Cancer.Dis Colon Rectum. 2020 Apr;63(4):441-449. doi: 10.1097/DCR.0000000000001597. Dis Colon Rectum. 2020. PMID: 31996582
-
Laparoscopic colectomy for cancer: an oncologic feasible option.Surg Oncol. 2000 Nov;9(3):127-34. doi: 10.1016/s0960-7404(01)00002-0. Surg Oncol. 2000. PMID: 11356341 Review.
-
Single-incision right hemicolectomy for malignancy: a feasible technique with standard laparoscopic instrumentation.Colorectal Dis. 2012 Nov;14(11):e764-70. doi: 10.1111/j.1463-1318.2012.03175.x. Colorectal Dis. 2012. PMID: 22776288 Review.
Cited by
-
Single-port versus multi-port laparoscopic surgery for colon cancer in elderly patients.Oncol Lett. 2016 Aug;12(2):1465-1470. doi: 10.3892/ol.2016.4802. Epub 2016 Jun 29. Oncol Lett. 2016. PMID: 27446454 Free PMC article.
-
Single-incision laparoscopic right colectomy in an unselected patient population.Surg Endosc. 2012 Jun;26(6):1595-601. doi: 10.1007/s00464-011-2076-4. Epub 2011 Dec 17. Surg Endosc. 2012. PMID: 22179463
-
Laparoendoscopic single-site surgery in gynecology: review of literature and available technology.J Minim Invasive Gynecol. 2011 Jan-Feb;18(1):12-23. doi: 10.1016/j.jmig.2010.07.013. Epub 2010 Oct 20. J Minim Invasive Gynecol. 2011. PMID: 20965792 Free PMC article. Review.
-
Single-incision plus one-port laparoscopic abdominoperineal resection with bilateral pelvic lymph node dissection for advanced rectal cancer: a case report.Int Surg. 2015 Jan;100(1):15-20. doi: 10.9738/INTSURG-D-14-00232.1. Int Surg. 2015. PMID: 25594635 Free PMC article.
-
Single-incision laparoscopic surgery using colon-lifting technique for colorectal cancer: a matched case-control comparison with standard multiport laparoscopic surgery in terms of short-term results and access instrument cost.Surg Endosc. 2012 May;26(5):1403-11. doi: 10.1007/s00464-011-2047-9. Epub 2011 Nov 20. Surg Endosc. 2012. PMID: 22101420
References
-
- Lacy AM, García-Valdecasas JC, Piqué JM, Delgado S, Campo E, Bordas JM, Taurá P, Grande L, Fuster J, Pacheco JL. Short-term outcome analysis of a randomized study comparing laparoscopic vs open colectomy for colon cancer. Surg Endosc. 1995;9:1101–1105. - PubMed
-
- Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, Heath RM, Brown JM. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol. 2007;25:3061–3068. - PubMed
-
- Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, Beart RW Jr, Hellinger M, Flanagan R Jr, Peters W, Nelson H. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg. 2007;246:655–62; discussion 662-664. - PubMed
-
- Whiteford MH, Denk PM, Swanström LL. Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc. 2007;21:1870–1874. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
