

PEEK cages as a potential alternative in the treatment of cervical spondylodiscitis: a preliminary report on a patient series
- PMID: 20069319
- PMCID: PMC2899978
- DOI: 10.1007/s00586-009-1265-5
PEEK cages as a potential alternative in the treatment of cervical spondylodiscitis: a preliminary report on a patient series
Abstract
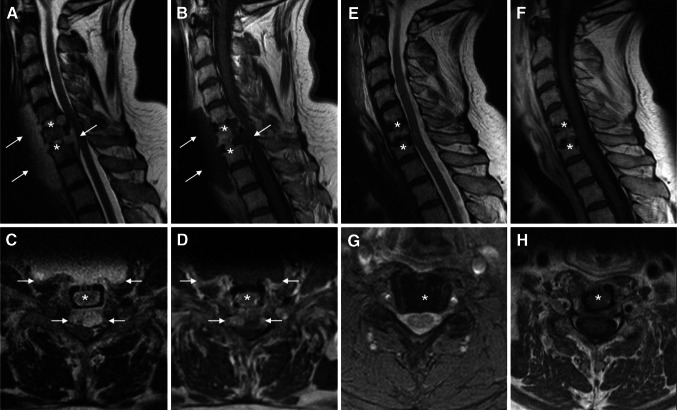
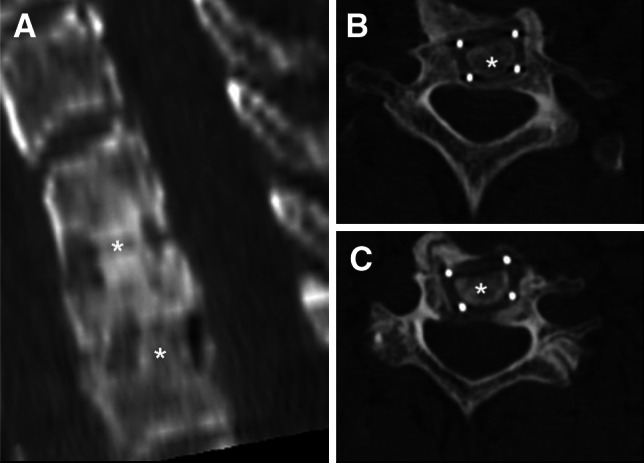
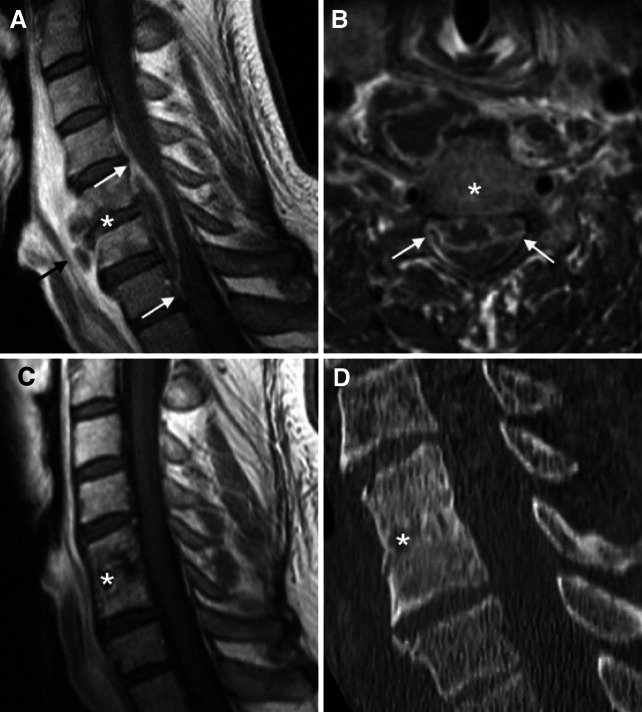
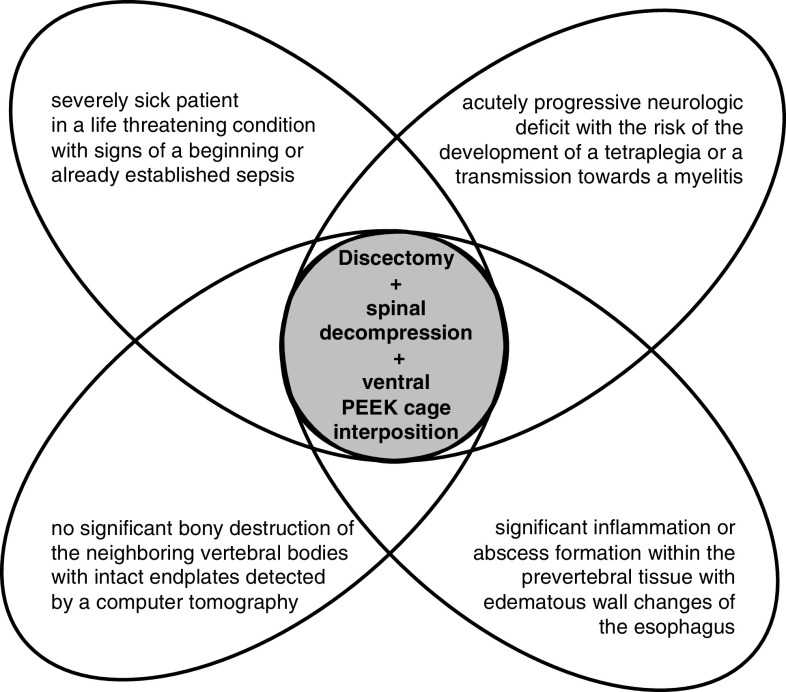
The surgical management of cervical spondylodiscitis consists of the resection of the affected disc, the decompression of the cervical spinal cord, followed by the stabilization using an autologous bone graft or a titanium implant combined with a ventral plate fixation. Until now, there were no studies about the practicability and putative safety of PEEK cages in cervical spine infection. Now, we present the history of five patients suffering from neurological deficits and septicemia caused by mono- or bisegmental pyogenic cervical discitis and intraspinal abscess without severe bone destruction. Patients were treated surgically by discectomy, decompression, and ventral spondylodesis. The disc was replaced by a PEEK cage without additional fixation. Progressive bony fusion and complete regression of the inflammatory changes was demonstrated 7-8 months later by a computer assisted tomography and contrast enhanced magnetic resonance imaging, respectively. The vertebral alignment changed minimally; the cages developed only a slight average subsidence. The clinical symptoms improved in all patients significantly. Neck pain or instability was never observed. Nevertheless, prospective investigations of a larger patient series are mandatory. We suppose that the use of PEEK cages represents a potential and safe alternative in the treatment of cervical spondylodiscitis in selected patients.
Figures
Similar articles
-
PEEK cage cervical ventral fusion in spondylodiscitis.Acta Neurochir (Wien). 2009 Nov;151(11):1537-41. doi: 10.1007/s00701-009-0486-z. Acta Neurochir (Wien). 2009. PMID: 19756355
-
Comparison of stand-alone polyetheretherketone cages and iliac crest autografts for the treatment of cervical degenerative disc diseases.Acta Neurochir (Wien). 2011 Jan;153(1):115-22. doi: 10.1007/s00701-010-0821-4. Epub 2010 Oct 6. Acta Neurochir (Wien). 2011. PMID: 20924769
-
Outcomes of interbody fusion cages used in 1 and 2-levels anterior cervical discectomy and fusion: titanium cages versus polyetheretherketone (PEEK) cages.J Spinal Disord Tech. 2010 Jul;23(5):310-6. doi: 10.1097/BSD.0b013e3181af3a84. J Spinal Disord Tech. 2010. PMID: 20124907
-
Anterior cervical fusion with polyetheretherketone (PEEK) cages in the treatment of degenerative disc disease. Preliminary observations in 36 consecutive cases with a minimum 12-month follow-up.Acta Neurochir (Wien). 2006 Mar;148(3):307-12; discussion 312. doi: 10.1007/s00701-005-0657-5. Epub 2005 Dec 12. Acta Neurochir (Wien). 2006. PMID: 16341633
-
Comparison of Clinical and Radiologic Outcomes Between Self-Locking Stand-Alone Cage and Cage with Anterior Plate for Multilevel Anterior Cervical Discectomy and Fusion: A Meta-Analysis.World Neurosurg. 2019 May;125:e117-e131. doi: 10.1016/j.wneu.2018.12.218. Epub 2019 Jan 21. World Neurosurg. 2019. PMID: 30677575
Cited by
-
[Gold standard for implant selection in operative therapy of spondylitis/spondylodiscitis].Orthopade. 2012 Sep;41(9):721-6. doi: 10.1007/s00132-012-1916-9. Orthopade. 2012. PMID: 22923160 German.
-
Minimally invasive management of cervical spondylodiscitis. A multicenter experience.Neurosurg Rev. 2025 Jan 8;48(1):29. doi: 10.1007/s10143-025-03191-z. Neurosurg Rev. 2025. PMID: 39779517
-
Cervical Pyogenic Spondylitis: A Comprehensive Review of Diagnosis and Treatment Strategy.J Clin Med. 2025 May 17;14(10):3519. doi: 10.3390/jcm14103519. J Clin Med. 2025. PMID: 40429514 Free PMC article. Review.
-
Polyetheretherketone (PEEK) for medical applications.J Mater Sci Mater Med. 2016 Jul;27(7):118. doi: 10.1007/s10856-016-5731-4. Epub 2016 Jun 3. J Mater Sci Mater Med. 2016. PMID: 27259708 Review.
-
Biomechanical evaluation and surface characterization of a nano-modified surface on PEEK implants: a study in the rabbit tibia.Int J Nanomedicine. 2014 Aug 14;9:3903-11. doi: 10.2147/IJN.S60387. eCollection 2014. Int J Nanomedicine. 2014. PMID: 25152620 Free PMC article.
References
-
- Korovessis P, Petsinis G, Koureas G, Iliopoulos P, Zacharatos S. Anterior surgery with insertion of titanium mesh cage and posterior instrumented fusion performed sequentially on the same day under one anesthesia for septic spondylitis of thoracolumbar spine: is the use of titanium mesh cages safe? Spine. 2006;31(9):1014–1019. doi: 10.1097/01.brs.0000215049.08622.9d. - DOI - PubMed
-
- Green S, Schlegel J (2001) Polymers for the medical industry. In: Conference Proceedings, Paper 2
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
