

Hemodynamic predictors of aortic dilatation in bicuspid aortic valve by velocity-encoded cardiovascular magnetic resonance
- PMID: 20070904
- PMCID: PMC2827385
- DOI: 10.1186/1532-429X-12-4
Hemodynamic predictors of aortic dilatation in bicuspid aortic valve by velocity-encoded cardiovascular magnetic resonance
Abstract
Background: Congenital bicuspid aortic valve (BAV) is a significant risk factor for serious complications including valve dysfunction, aortic dilatation, dissection, and sudden death. Clinical tools for identification and monitoring of BAV patients at high risk for development of aortic dilatation, an early complication, are not available.
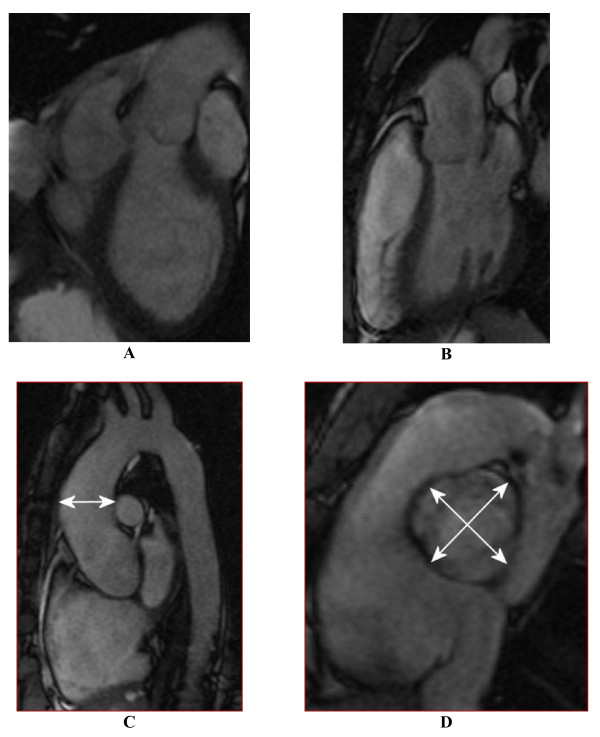
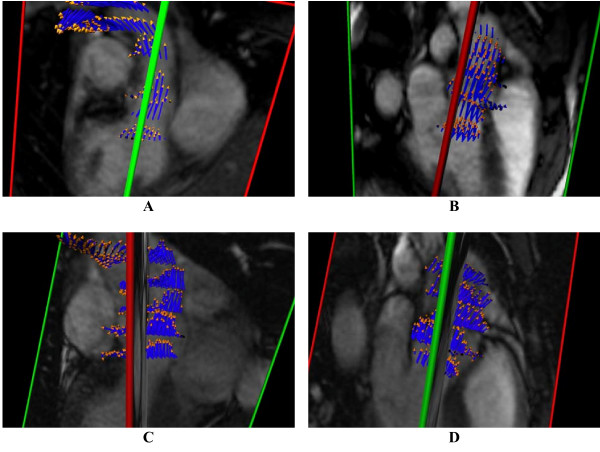
Methods: This paper reports an investigation in 18 pediatric BAV patients and 10 normal controls of links between abnormal blood flow patterns in the ascending aorta and aortic dilatation using velocity-encoded cardiovascular magnetic resonance. Blood flow patterns were quantitatively expressed in the angle between systolic left ventricular outflow and the aortic root channel axis, and also correlated with known biochemical markers of vessel wall disease.
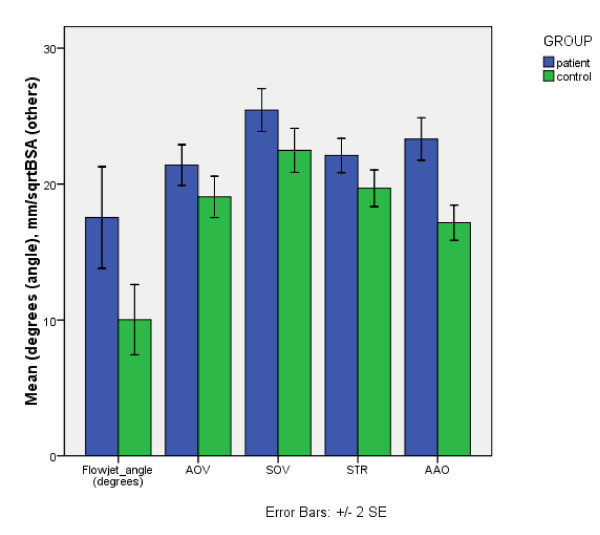
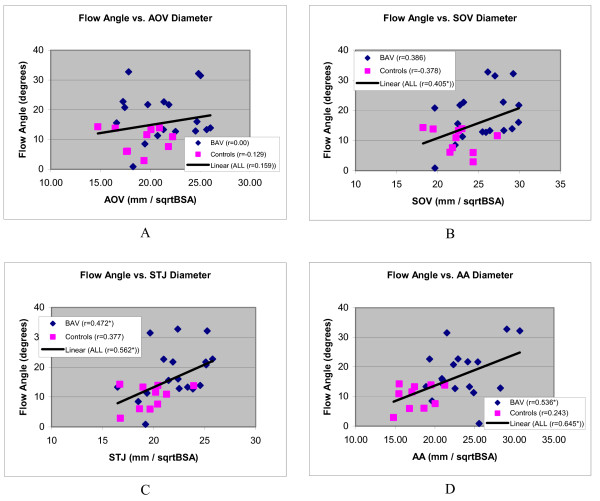
Results: The data confirm larger ascending aortas in BAV patients than in controls, and show more angled LV outflow in BAV (17.54 +/- 0.87 degrees) than controls (10.01 +/- 1.29) (p = 0.01). Significant correlation of systolic LV outflow jet angles with dilatation was found at different levels of the aorta in BAV patients STJ: r = 0.386 (N = 18, p = 0.048), AAO: r = 0.536 (N = 18, p = 0.022), and stronger correlation was found with patients and controls combined into one population: SOV: r = 0.405 (N = 28, p = 0.033), STJ: r = 0.562 (N = 28, p = 0.002), and AAO r = 0.645 (N = 28, p < 0.001). Dilatation and the flow jet angle were also found to correlate with plasma levels of matrix metallo-proteinase 2.
Conclusions: The results of this study provide new insights into the pathophysiological processes underlying aortic dilatation in BAV patients. These results show a possible path towards the development of clinical risk stratification protocols in order to reduce morbidity and mortality for this common congenital heart defect.
Figures

References
-
- Yener N, Oktar GL, Erer D, Yardimci MM, Yener A. Bicuspid aortic valve. Ann Thorac Cardiovasc Surg. 2002;8:264–267. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
